

More details emerge on why the mRNA vaccines are not preventing Omicron infection
Robert W Malone MD, MS
I must be confused. Please remind me, why is there unanimous agreement by the empaneled expert vaccine thought leaders who provide independent oversight of the FDA and CDC review process for SARS-CoV-2 vaccination, that very young children who are at their peak period for thymic development and maturation, should be administered genetic vaccines encoding a viral antigen derived from a largely extinct viral strain? Particularly when the data concerning the role of immune imprinting on development of viral escape and negative vaccine effectiveness against the Omicron variants are becoming so compelling?
This is going to get a bit technical, so I suggest that you take a moment to go get a cup of coffee or tea before launching into this one. I will do my best to make it understandable, but immunology and virology can get a bit complicated, and I will bypass many of the nuances for the sake of brevity and comprehension.
From the standpoint of the approved narrative, at this point in time (June 2022) one of the major unresolved COVIDcrisis mysteries has been why so many who are “fully vaccinated” (whatever that means) against SARS-CoV-2 are still developing infection and COVID disease. Celebrity examples illustrating the point include vaccine mandate advocate Canadian Prime Minister Justin Trudeau, who was infected (despite apparently being fully vaccinated) late during the initial Omicron wave (January 27, 2022), and now has been re-infected (after receiving three doses of the mRNA inoculum) on June 13, 2022 (four months, 18 days later). Dr. Anthony Fauci provides another recent example. Despite having received four doses of the mRNA inoculum, he was infected and developed COVID disease in mid-June, 2022. Vaccine mandate advocate California Governor Gavin Newsom, just 10 days after his fourth inoculum, also was infected and developed COVID. Notice a pattern?
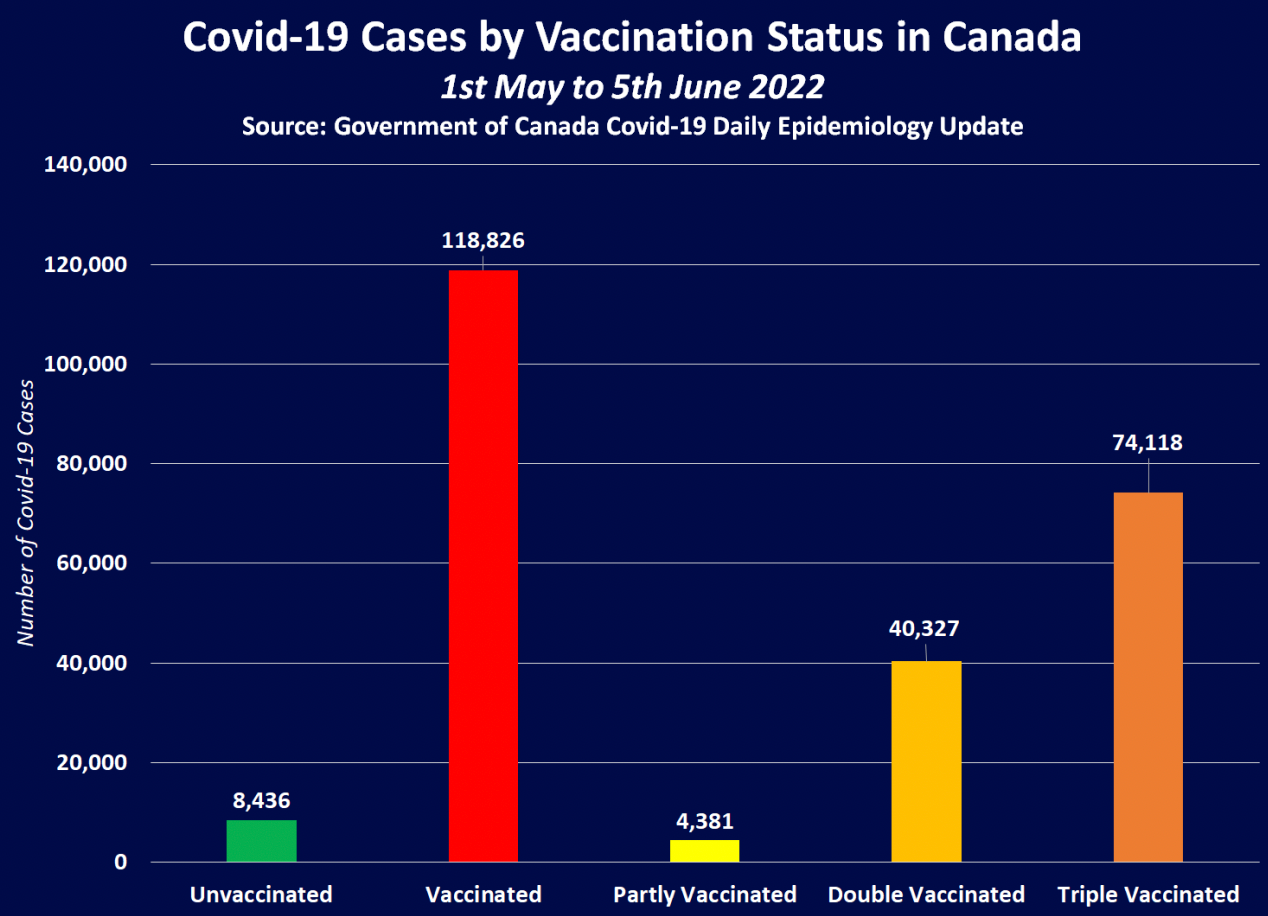
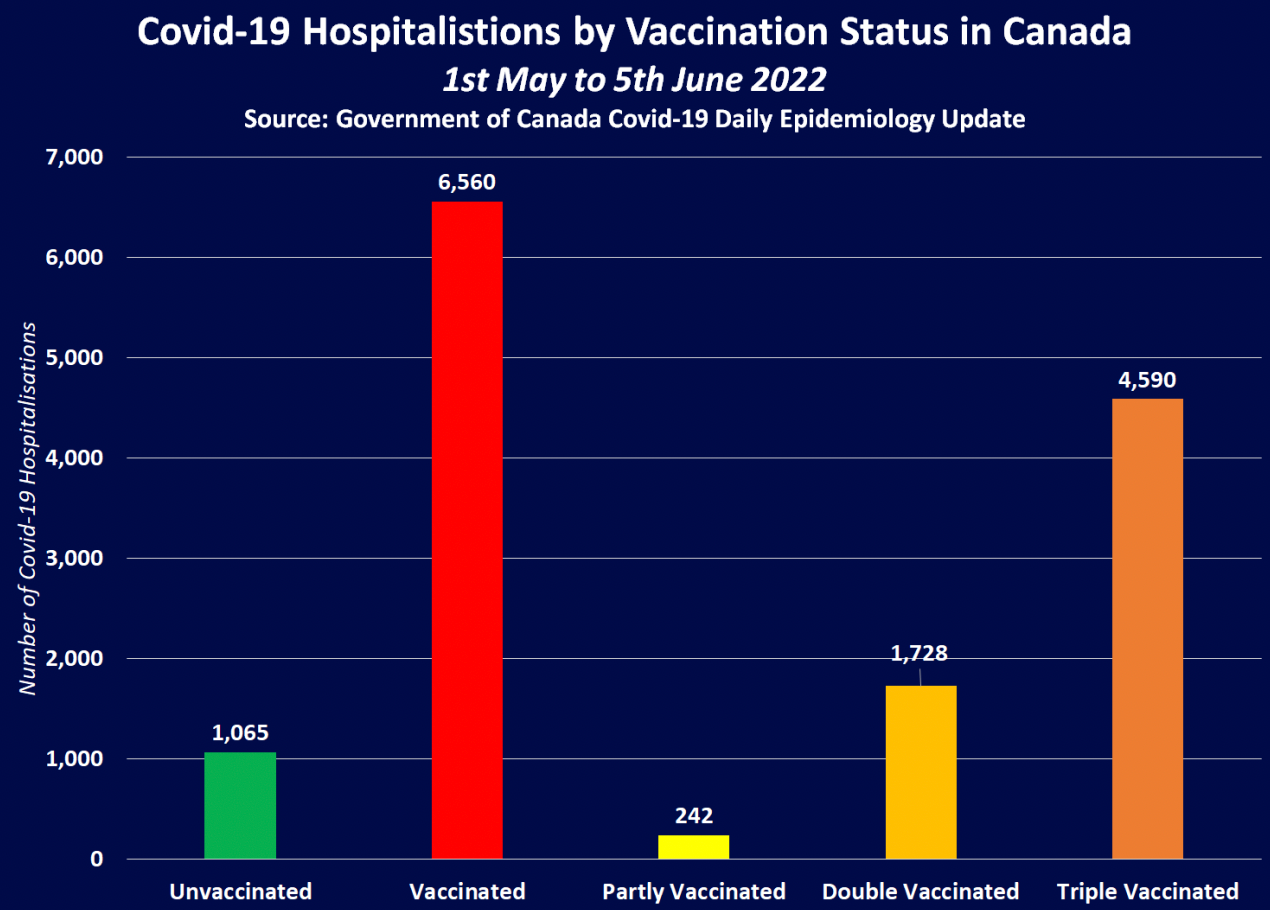
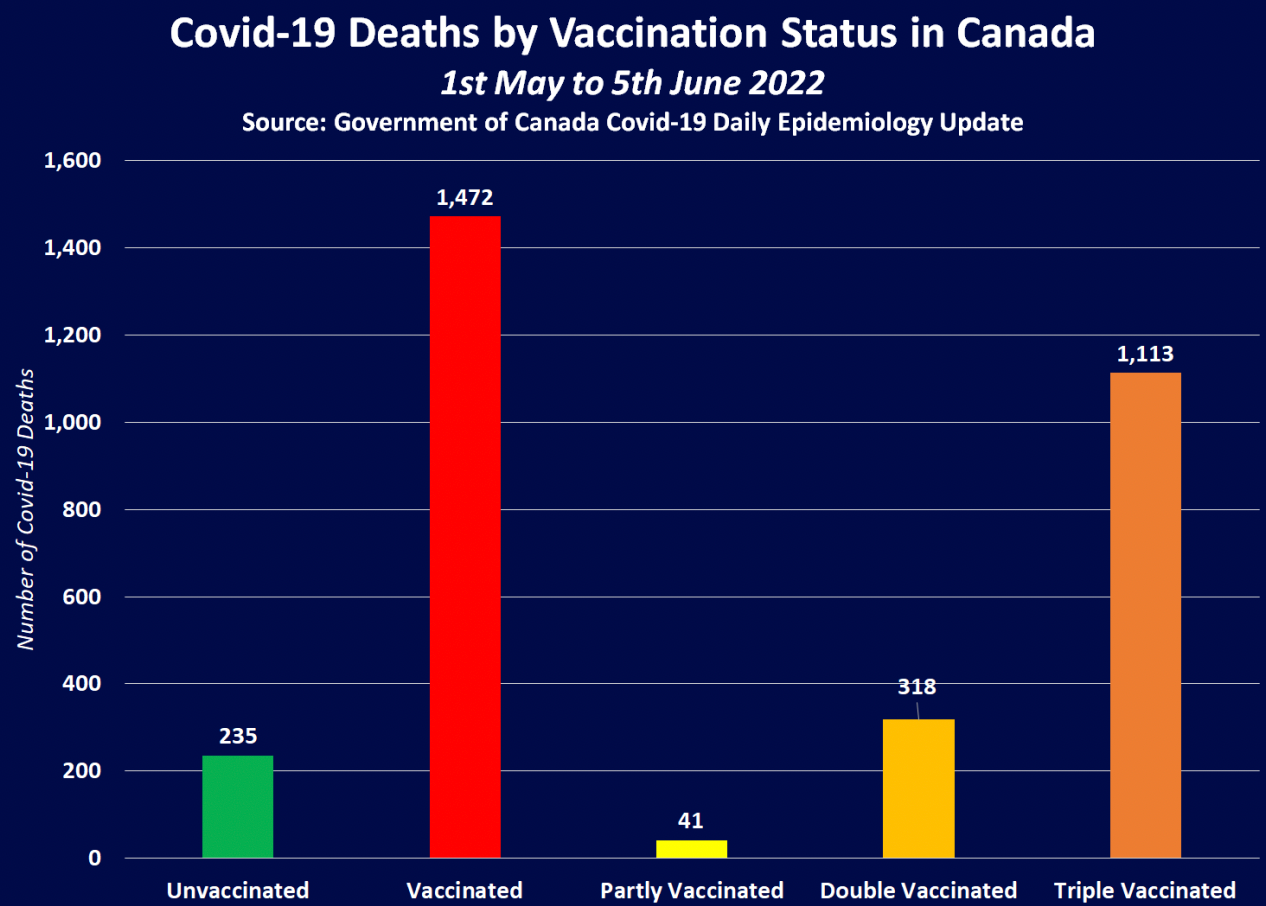
In many countries, data during the first two quarters of 2022 indicate that the majority of individuals identified as hospitalized due to COVID are “fully vaccinated”. Of course, in most western countries, there are more vaccinated than unvaccinated individuals, so this general finding requires some qualification and correction for the resulting sampling bias. To provide one example to illustrate the point, on February 01, 2022 the Canadian COVID Care Alliance distributed a video documenting the propaganda around the Myth of A Pandemic of the Unvaccinated which documents this fact in the context of Ontario, Canada-derived public health data. As discussed in the video, many of these data point towards “negative effectiveness” of the genetic vaccines – meaning that those who are “fully vaccinated” are MORE likely to get COVID disease than those who are “unvaccinated”. A word of caution about this conclusion; the term “unvaccinated” is increasingly misleading, as over time a larger and larger fraction of the total population has become infected, and so has not only been previously infected (and immunologically primed) by infection with one or more of the seasonal “cold” betacoronaviruses (which share large numbers of both B and T cell epitope antigens with SARS-CoV-2), but have also been “boosted” by natural infection with one of the variants of SARS-CoV-2. This problem (or artifact) has become increasingly true since the onset of the Omicron variant. For example, see this summary of Canadian COVID-19 associated total cases, hospitalized cases and deaths which have accrued between May 01, 2022 and June 05, 2022. Fully Vaccinated patients account for 9 in every 10 COVID-19 Deaths in Canada over the past month; 4 in every 5 of which had received three inoculations. Most people know from their own personal experiences that whether or not close associates, family, friends or themselves have been previously infected OR vaccinated (or both), they are highly likely to also get infected by the Omicron (or Pango lineage B.1.1.529) variant of SARS-CoV-2.
Just to be crystal clear on this point, as I said on the steps of the Lincoln Memorial on January 23, 2022;
“Regarding the genetic COVID vaccines, the science is settled.
They are not working, and they are not completely safe.
Now we have Omicron. These vaccines were designed for the Original Wuhan strain, a different virus. Whether they made sense for protecting our elderly and frail from the original virus is irrelevant. So let’s stop arguing about that. We must look forward.
These vaccines do not prevent Omicron infection, viral replication, or spread to others. In our daily lives, with our friends, with our families, we all know that this is true.
These genetic vaccines are leaky, have poor durability, and even if every man, woman, and child in the United States were vaccinated, these products cannot achieve herd immunity and stop COVID. They are not completely safe, and the full nature of the risks remain unknown.”
The Washington Post called me a liar and spreader of discredited misinformation at the time for making this statement, but since then this has become a widely accepted scientific truth, one which is truly self-evident to virtually anyone who is not caught up in the Mass Formation Psychosis process. My sin which triggered the defamation was apparently stating an inconvenient truth before it became widely accepted.
See for example:
Effectiveness of BNT162b2 vaccine against omicron variant in South Africa. S. Collie, J. Champion, H. Moultrie, L.-G. Bekker, G. Gray, N. Engl. J. Med.386, 494–496 (2022)
Effectiveness of mRNA-1273 against SARS-CoV-2 Omicron and Delta variants. H. F. Tseng, B. K. Ackerson, Y. Luo, L. S. Sy, C. A. Talarico, Y. Tian, K. J. Bruxvoort, J. E. Tubert, A. Florea, J. H. Ku, G. S. Lee, S. K. Choi, H. S. Takhar, M. Aragones, L. Qian, Nat. Med.28, 1063–1071 (2022).
Covid-19 vaccine effectiveness against the omicron (B.1.1.529) variant. N. Andrews, J. Stowe, F. Kirsebom, S. Toffa, T. Rickeard, E. Gallagher, C. Gower, M.Kall, N. Groves, A. M. O’Connell, D. Simons, P. B. Blomquist, A. Zaidi, S. Nash, N.Iwani Binti Abdul Aziz, S. Thelwall, G. Dabrera, R. Myers, G. Amirthalingam, S. Gharbia, J. C. Barrett, R. Elson, S. N. Ladhani, N. Ferguson, M. Zambon, C. N. J.Campbell, K. Brown, S. Hopkins, M. Chand, M. Ramsay, J. Lopez Bernal, N. Engl. J. Med.386, 1532–1546 (2022)
Omicron escapes the majority of existing SARS-CoV-2 neutralizing antibodies. Cao Y, Wang J, Jian F, Xiao T, Song W, Yisimayi A, Huang W, Li Q, Wang P, An R, Wang J, Wang Y, Niu X, Yang S, Liang H, Sun H, Li T, Yu Y, Cui Q, Liu S, Yang X, Du S, Zhang Z, Hao X, Shao F, Jin R, Wang X, Xiao J, Wang Y, Xie XS.Nature. 2022 Feb;602(7898):657-663. doi: 10.1038/s41586-021-04385-3. Epub 2021 Dec 23.PMID: 35016194
Omicron variant susceptibility to neutralizing antibodies induced in children by natural SARS-CoV-2 infection or COVID-19 vaccine. Chen LL, Chua GT, Lu L, Chan BP, Wong JS, Chow CC, Yu TC, Leung AS, Lam SY, Wong TW, Tsang HW, Wong IC, Chan KH, Yuen KY, Ip P, Kwan MY, To KK.Emerg Microbes Infect. 2022 Dec;11(1):543-547. doi: 10.1080/22221751.2022.2035195.PMID: 35084295
The Omicron variant is highly resistant against antibody-mediated neutralization: Implications for control of the COVID-19 pandemic. Hoffmann M, Krüger N, Schulz S, Cossmann A, Rocha C, Kempf A, Nehlmeier I, Graichen L, Moldenhauer AS, Winkler MS, Lier M, Dopfer-Jablonka A, Jäck HM, Behrens GMN, Pöhlmann S.Cell. 2022 Feb 3;185(3):447-456.e11. doi: 10.1016/j.cell.2021.12.032. Epub 2021 Dec 24.PMID: 35026151
It goes on and on. I think we can now safely say that it was the Washington Post who was peddling mis- or dis-information (or just plain old fashioned propaganda) in the case of their defamatory article attacking me.
Previously, the potential for negative effectiveness of the vaccines was actively denied by researchers involved in the design and creation of the genetic vaccines, but unfortunately data and the passage of time has proven their assertions of safety to have been premature. So much for such highly confident “experts”, their predictive powers of inference, and their personal hubris.
There are multiple working hypothesis for why there is the appearance of negative effectiveness of these genetic inoculations for preventing COVID-19 disease. Examples include;
- Antibody Dependent Enhancement (ADE).
- Other forms of Vaccine-enhanced Disease (VAED).
- Vaccine-induced acquired immunodeficiency (VAIDS) of one type or another.
- Evolution of SARS-CoV-2 in the context of widely deployed leaky vaccines to select for variants which will escape the pressure of vaccine-induced immune responses.
- Antigenic or immune imprinting, otherwise known as “Original Antigenic Sin”.
I am sure that there are many more hypotheses, and it is always important to recognize that more than one thing can be going on at the same time. However, the preponderance of data increasingly point to immune imprinting/Original Antigenic Sin as the leading explanation for the observed public health data suggesting negative effectiveness of the mRNA inoculations which are currently being marketed as vaccines, but which (with recommendations for four or more doses) are functionally being deployed more as immuno-therapeutics.
Of course the corporate media, completely unaware or in denial of their profound ignorance and incompetence as objective mediators of scientific discussions regarding complicated immunologic topics, has once again interjected its pro-vax, aggressively-deny-any-problems agenda into the whole discussion. And then, once again, there are the scientifically unqualified “factcheckers”. But by now, that is a routine business practice which is to be expected.
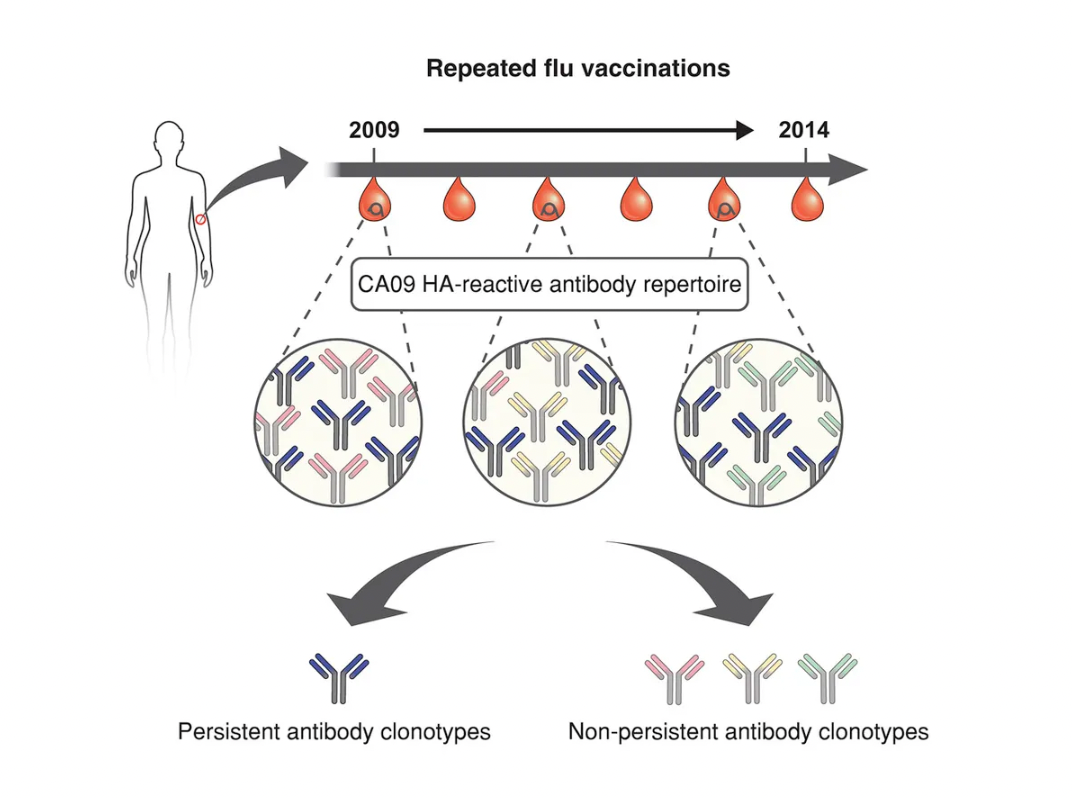
So what is immune imprinting or “original antigenic sin”? Here is one explanation from a group of influenza virus researchers, investigating differently immunologically biased age groups in their responses to different influenza virus groups (clades):
“We define immune imprinting as a lifelong bias in immune memory of, and protection against, the strains encountered in childhood. Such biases most likely become entrenched as subsequent exposures back-boost existing memory responses, rather than stimulating de novo responses [1]. By providing particularly robust protection against certain antigenic subtypes, or clades, imprinting can provide immunological benefits, but perhaps at the cost of equally strong protection against variants encountered later in life.”
Here is the reference [1] that they are citing above, for those who are passionate about following all the leads down the various rabbit holes. This reference nicely addresses the use and limitations of the two terms “immune imprinting” and “original antigenic sin”, finding the former term a generally better fit to the actual data than the latter:
From Original Antigenic Sin to the Universal Influenza Virus Vaccine. Henry C, Palm A-KE, Krammer F, Wilson PC. Trends Immunol. 2018;39: 70–79.
The authors of this article provide a very nice summary of the issues at hand, which are also directly applicable to coronavirus vaccines and evolved SARS-CoV-2 variants:
“Antibody responses are essential for protection against influenza virus infection. Humans are exposed to a multitude of influenza viruses throughout their lifetime and it is clear that immune history influences the magnitude and quality of the antibody response. The ‘original antigenic sin’ concept refers to the impact of the first influenza virus variant encounter on lifelong immunity. Although this model has been challenged since its discovery, past exposure, and likely one’s first exposure, clearly affects the epitopes targeted in subsequent responses. Understanding how previous exposure to influenza virus shapes antibody responses to vaccination and infection is critical, especially with the prospect of future pandemics and for the effective development of a universal influenza vaccine.”
Getting to the point, the data concerning the “how” and “why” of this odd and unfortunate relationship between the SARS-CoV-2 genetic vaccines, viral evolution of immune escape mutants, and negative effectiveness are really starting to come into focus. It does appear that immune imprinting is playing a big role, but also that it is not the general vaccinated population but rather the subset of people who develop chronic infections with SARS-CoV-2 who are the ones driving development of the antibody escape mutant viruses. And it is certainly not the general unvaccinated population, to the extent that there even are any individuals (other than newborn infants) who are immunologically naive to SARS-CoV-2. And speaking of the newborns, the data concerning immune imprinting demonstrate that vaccinating very young children with a genetic vaccine which expresses a Spike antigen from a virus that has not been circulating for a very long time (with the consequent immune imprinting) is either malevolent or madness or both.
It can take a long time and often requires interactions between many different people, together with quite a bit of trial and error, to get to the bottom of complicated problems. This is generally true in science as well as in life. Which makes the rapid progress towards understanding the immunologic and virological processes which are driving the negative effectiveness of the genetic vaccines and immune escape from vaccine-induced protection by SARS-CoV-2 all the more remarkable.
Examples of relevant scientific literature include the following (note the progression from smaller, more fringe journals to mainstream):
Original Antigenic Sin: the Downside of Immunological Memory and Implications for COVID-19. Brown EL, Essigmann HT.mSphere. 2021 Mar 10;6(2):e00056-21. doi: 10.1128/mSphere.00056-21.PMID: 33692194
Evidence for Deleterious Antigenic Imprinting in SARS-CoV-2 Immune Response. Sen SR, Sanders EC, Santos AM, Bhuvan K, Tang DY, Gelston AA, Miller BM, Ricks-Oddie JL, Weiss GA.bioRxiv. 2021 Jun 9:2021.05.21.445201. doi: 10.1101/2021.05.21.445201. Preprint.PMID: 34127968
Immune imprinting and SARS-CoV-2 vaccine design. Wheatley AK, Fox A, Tan HX, Juno JA, Davenport MP, Subbarao K, Kent SJ.Trends Immunol. 2021 Nov;42(11):956-959. doi: 10.1016/j.it.2021.09.001. Epub 2021 Sep 15.PMID: 34580004
Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Röltgen K, Nielsen SCA, Silva O, Younes SF, Zaslavsky M, Costales C, Yang F, Wirz OF, Solis D, Hoh RA, Wang A, Arunachalam PS, Colburg D, Zhao S, Haraguchi E, Lee AS, Shah MM, Manohar M, Chang I, Gao F, Mallajosyula V, Li C, Liu J, Shoura MJ, Sindher SB, Parsons E, Dashdorj NJ, Dashdorj ND, Monroe R, Serrano GE, Beach TG, Chinthrajah RS, Charville GW, Wilbur JL, Wohlstadter JN, Davis MM, Pulendran B, Troxell ML, Sigal GB, Natkunam Y, Pinsky BA, Nadeau KC, Boyd SD.Cell. 2022 Mar 17;185(6):1025-1040.e14. doi: 10.1016/j.cell.2022.01.018. Epub 2022 Jan 25.PMID: 35148837
Cellular and Humoral Immune Responses in Covid-19 and Immunotherapeutic Approaches. Hasan A, Al-Ozairi E, Al-Baqsumi Z, Ahmad R, Al-Mulla F.Immunotargets Ther. 2021 Mar 9;10:63-85. doi: 10.2147/ITT.S280706. eCollection 2021.PMID: 33728277
Immunological imprinting of the antibody response in COVID-19 patients. Aydillo T, Rombauts A, Stadlbauer D, Aslam S, Abelenda-Alonso G, Escalera A, Amanat F, Jiang K, Krammer F, Carratala J, García-Sastre A.Nat Commun. 2021 Jun 18;12(1):3781. doi: 10.1038/s41467-021-23977-1.PMID: 34145263
Imprinted SARS-CoV-2-specific memory lymphocytes define hybrid immunity. Rodda LB, Morawski PA, Pruner KB, Fahning ML, Howard CA, Franko N, Logue J, Eggenberger J, Stokes C, Golez I, Hale M, Gale M Jr, Chu HY, Campbell DJ, Pepper M.Cell. 2022 Apr 28;185(9):1588-1601.e14. doi: 10.1016/j.cell.2022.03.018. Epub 2022 Mar 17.PMID: 35413241
BA.2.12.1, BA.4 and BA.5 escape antibodies elicited by Omicron infection. Cao Y, et al. Nature. 2022. PMID: 35714668
With the above prelude in mind, you should now be ready for a discussion of the following peer-reviewed publication, in which I particularly appreciate finding a detailed recognition and discussion that protection against SARS-CoV-2 involves both an antibody/B cell as well as a T cell component:
Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure
Catherine J Reynolds, Corinna Pade, Joseph M Gibbons et al. Science, 2022 Jun 14; PMID: 35699621 , DOI: 10.1126/science.abq1841
The abstract does meet the criteria for “bombshell” in my opinion.
“The Omicron, or Pango lineage B.1.1.529, variant of SARS-CoV-2 carries multiple spike mutations with high transmissibility and partial neutralizing antibody (nAb) escape. Vaccinated individuals show protection from severe disease, often attributed to primed cellular immunity. We investigated T and B cell immunity against B.1.1.529 in triple mRNA vaccinated healthcare workers (HCW) with different SARS-CoV-2 infection histories. B and T cell immunity against previous variants of concern was enhanced in triple vaccinated individuals, but magnitude of T and B cell responses against B.1.1.529 spike protein was reduced. Immune imprinting by infection with the earlier B.1.1.7 (Alpha) variant resulted in less durable binding antibody against B.1.1.529. Previously infection-naïve HCW who became infected during the B.1.1.529 wave showed enhanced immunity against earlier variants, but reduced nAb potency and T cell responses against B.1.1.529 itself. Previous Wuhan Hu-1 infection abrogated T cell recognition and any enhanced cross-reactive neutralizing immunity on infection with B.1.1.529.”
Big Bada boom. Short version, I think that what the authors are saying is that Omicron is evolving to not only escape prior neutralizing antibodies generated from either vaccination (with spike protein derived from Wuhan Hu-1) or infection with Wuhan Hu-1 OR B.1.1.7 (Alpha), but infection with Omicron variant B.1.1.529 is reducing both T cell and B cell (antibody) responses to itself. This is not good news.
Let’s start with the introduction and background section in Part 1 so that we can better understand the findings in this paper, and then move on to the research and conclusions in Part 2.
“Across several studies, 2 or 3-dose vaccination is protective against severe disease and hospitalization, albeit with poor protection against transmission.”
Actually, the references cited by the authors demonstrate that, in a time dependent manner, the effectiveness against severe disease and hospitalization is in the 40% – 70% range. Which means that 30% to 60% of fully vaccinated persons were NOT protected against hospitalization. Based on this, my conclusion is that the genetic vaccines are not even working well to prevent hospitalization – and Omicron yields mild COVID disease. “Working well” or “Not working” is a subjective matter, so to you factcheckers reading this, please bugger off.
“A rationale for this high rate of breakthrough infections comes from mapping of virus neutralization using either post-vaccination immune sera or monoclonal antibodies, showing this to be the most antibody immune-evasive VOC, with titers generally reduced by 20-40-fold.”
Here are the references cited to support this statement.
Considerable escape of SARS-CoV-2 Omicron to antibody neutralization. D. Planas, N. Saunders, P. Maes et al. , Nature 602, 671–675 (2022).
Striking antibody evasion manifested by the Omicron variant of SARS-CoV-2. L. Liu, S. Iketani, Y. Guo, et al., Nature 602, 676–681 (2022).
Omicron extensively but incompletely escapes Pfizer BNT162b2 neutralization. S. Cele, L. Jackson, D. S. Khoury, et al., Nature 602, 654–656 (2022).
Neutralization of SARS-CoV-2 Omicron by BNT162b2 mRNA vaccine-elicited human sera. A. Muik, B. G. Lui, A. K. Wallisch, et al., Science 375, 678–680 (2022).
I think that you can see the trend here. And suffice to say, it is not supporting the position taken by the Washington Post.
“The relative attenuation of severe symptoms in vaccinated compared to unvaccinated groups is likely attributable to the partial protection conferred by the residual neutralizing Ab (nAb) repertoire and the activation of primed B cell and T cell memory.”
Now we are focusing on T cell rather than B cell (antibody)-based immune responses. Note the cautious wording? Are the “unvaccinated” groups in question immunologically naive? Is there a comparison to naturally infected patients? Let’s look at the references cited.
SARS-CoV-2 vaccination induces immunological T cell memory able to cross-recognize variants from Alpha to Omicron. A. Tarke, C. H. Coelho, Z. Zhang, et al, Cell 185, 847–859.e11 (2022).
-The control group here was previously infected individuals who had mild disease.
Ancestral SARS-CoV-2-specific T cells cross-recognize the Omicron variant. Y. Gao, C. Cai, A. Grifoni, et al, Nat. Med.28, 472–476 (2022).
-This does include infected and vaccinated, and shows a relatively lower drop in preservation of T cell cross recognition in vaccinated versus infected, but does appear to me to directly compare these numbers statistically.
Vaccines elicit highly conserved cellular immunity to SARS-CoV-2 Omicron. J. Liu, A. Chandrashekar, D. Sellers, et al, Nature 603, 493–496 (2022).
-This study does not compare vaccinated versus naturally infected, and although it asserts that the vaccines provide substantial protection from Omicron, it does not demonstrate this in any way other than showing persistence of T cell responses.
T cell reactivity to the SARS-CoV-2 Omicron variant is preserved in most but not all individuals. V. Naranbhai, A. Nathan, C. Kaseke, et al, Cell 185, 1041–1051.e6 (2022).
-This study examines both natural infection and vaccinated individuals, and demonstrates that in most patients from either category, T cell responses are relatively preserved against Omicron. But there is a caveat – there is a subset of patients who are losing T cell responses to Omicron, in addition to losing B cell (antibody) responses. This may explain the patients who report repeated or chronic Omicron infection, and who may be the ones that are driving the further development of escape mutant viruses.
“However, examination of individual responses revealed that a distinct proportion of individuals with prior infection and/or vaccination have substantially reduced T cell reactivity to Omicron (but not Delta). Further evaluation of spike-specific CD4+ and CD8+ memory T cell responses revealed a significant difference in CD8+ T cell proliferation in response to Omicron spike relative to wild type. In sum, T cell reactivity to the SARS-CoV-2 Omicron variant was preserved in most but not all prior infected and vaccinated individuals.”
T cell responses to SARS-CoV-2 spike cross-recognize Omicron. R. Keeton, M. B. Tincho, A. Ngomti, R. Baguma, et al, Nature 603, 488–492 (2022).
-This study examines both vaccinated and naturally infected patients, and in contrast to many of the prior reports relative preservation of T cell responses in both categories of patients. The authors conclude that:
“It remains to be determined whether well-preserved T cell immunity to Omicron contributes to protection from severe COVID-19 and is linked to early clinical observations from South Africa and elsewhere.”
Efficient recall of Omicron-reactive B cell memory after a third dose of SARS-CoV-2 mRNA vaccine. R. R. Goel, M. M. Painter, K. A. Lundgreen, et al., Cell 185, 1875–1887.e8 (2022).
-This study just focused on memory B cells (which is not easy to do) over time in vaccinated individuals. No assessment of naturally infected/immune patients. Their findings also varied from some of the above, but they had some interesting observations:
“Omicron-binding memory B cells were efficiently reactivated by a 3rd dose of wild-type vaccine and correlated with the corresponding increase in neutralizing antibody titers. In contrast, pre-3rd dose antibody titers inversely correlated with the fold-change of antibody boosting, suggesting that high levels of circulating antibodies may limit the added protection afforded by repeat short interval boosting.”
So we can conclude from this study that the timing of boosting is important. Too late, and you become as or more susceptible to infection and disease than the naturally infected. Too early, and the antibodies still circulating from the prior inoculation will interfere with the boost. Good to know, if you are someone
Part 2 will review the specific studies and findings reported by this Imperial College, UK team in their Science publication “Immune boosting by B.1.1.529 (Omicron) depends on previous SARS-CoV-2 exposure”. In this study, all patients were vaccinated with up to three doses of Comirnaty.
Content retrieved from: https://rwmalonemd.substack.com/p/immune-imprinting-comirnaty-and-omicron?utm_source=substack&utm_medium=email.