While censoring positive studies of ivermectin, the journals published fraudulent studies to try to “prove” ivermectin was ineffective. It is a well-known Disinformation tactic called “The Fake.”
Ok, so where were we? Oh yeah, I recently covered the rejections and retractions of positive ivermectin studies by the Editorial Mafia that control the high-impact medical journals. Now let’s go over the trials that they did publish on ivermectin. Note the very first play from the Disinformation Playbook, a tactic created and perfected by the Tobacco Industry over decades:
The obverse of censorship is propaganda (or vice versa) as Professor Marc Crispin Miller says. Big Pharma Disinformation campaigns against repurposed drugs in COVID employed both tactics equally. Again, I have already detailed the high-impact journal censorship of studies supporting repurposed medicines in this 3 part series.
Professor Miller’s definition of propaganda is “a story or message that gets you to think or act in a certain way.” In this post I want to focus on how all the propaganda used to steer the U.S population away from ivermectin was created. None of it would have been possible without the complicity of the high-impact medical journals. It laid the foundation upon which all the propaganda rested upon. None of it would have been possible without first establishing “the Science” showing ivermectin to be ineffective. This was established solely via the high impact journal publication of fraudulent and/or severely/willfully flawed studies.
Remember, the entire objective of Big Pharma Disinformation campaigns is to counteract “science that emerges which is inconvenient to Industry interests.” The tactics to accomplish this was invented by a PR firm working for Big Tobacco in the 1950’s. That PR firm still exists today. No wonder that PR firm still thrives. They literally were able to suppress and distort the evidence of lethality and toxicity of tobacco for 50 years in the service of that Industry. That “science” supported an insane winning streak in lawsuits against them for 40 years, until they finally succumbed with the 1998 “Master Settlement Agreement” reached with the attorney generals of 46 states, putting an end to a lot of their malevolent chicanery (but not really).
Big Pharma learned from Big Tobacco that you can prevent ivermectin science from emerging by censoring the “inconveniently positive” studies while only publishing “conveniently negative” studies, you could destroy the idea that repurposed drugs are effective in the pandemic. I have said it many times but never have two generic drugs (HCQ and IVM) presented a greater threat to their goals and profits within the largest new marketplace that has ever been created for their products.
The “negative” studies they published are what fueled the massive media and health agency Disinformation campaigns (false narratives) against ivermectin. Make a special note of how to identify “narratives,” i.e propaganda campaigns. A friend of mine has a rule he calls the “2 by 4.” If the story runs for 2 weeks on 4 different media or TV channels, not only is it a narrative (not always a false one but rarely if ever totally accurate) but more importantly, it is what takes hold of the minds of the majority of the country and becomes “mainstream” thinking. 2 by 4. Remember that. Although not every one of these trials triggered a 2 by 4, each time the papers and television stations across the world trumpeted the “negative” study results over at least the next several days after publication. The real “2 x4” propaganda campaign was the “horse dewormer” one which was triggered, not by a publication, but by a massive rise in U.S ivermectin prescriptions in mid-August of 2021. More on that soon.
The propaganda was disseminated to the average citizen through major (corporate/legacy) media, and to the physicians and health systems through the high-impact medical journals. Let’s not forget that physicians also consume lots of media so they were double whammy’ed and thus became some of the most ferocious attackers of “ivermectin advocates.” Poor things. Me and the FLCCC were initially hurt by these attacks, but that feeling quickly turned to a deep sadness as we watched medical professionals the world over act out against ivermectin after being fed outrageous “scientific” lies. I must say that the despair I felt over their behavior paled in comparison to how I felt over their vaccine behavior, none more so than when doctors across the world literally mandated and/or strongly recommended vaccinating people who had just recovered from the disease they were vaccinating against. Using the most lethal and toxic medical intervention in modern history. Let’s not go there right now.
The publication of the numerous fraudulent or severely flawed studies supposedly “proving” ivermectin ineffective in COVID then launched massive negative PR campaigns using almost every communication medium possible – social media, newspapers, radio, televisions news programs, late night talk shows etc. They all told identical “stories” or “narratives.” The average American citizen (and physician) reading or listening to these stories found their thoughts directed as follows;
- Ivermectin is a dangerous medication suitable only for deworming horses.
- Positive studies of ivermectin were all low quality, poorly designed, or outright fraudulent and thus cannot be trusted.
- The only positive ivermectin studies occurred in areas where parasitic infections were endemic.
- Physicians claiming ivermectin is effective do not know how to interpret studies correctly and rely on “bad science.”
- Physicians cannot tell if a drug they gave to a patient with an acute viral syndrome is effective unless an RCT is done to “prove it.”
- Ivermectin “advocates” are ignorant of the “real Science” and thus have a religious or political belief in the medicine rather than a scientific one.
- Those who interpret ivermectin studies as supporting its use in COVID are misguided, not credible, ignorant, or are “anti-vax” conspiracy theorists.
- In contrast to the low quality studies showing ivermectin to be effective, the “real” studies, i.e. “well-designed,” “rigorous,” “large,” “properly done” trials instead proved it is ineffective in the treatment of COVID.
- That studies of its use in prevention should be ignored since the vaccines have already been proven to be “safe and effective.”
All of the above engendered “thoughts” quickly directed people’s actions in the following ways;
- Made health care providers refrain from treating COVID patients with ivermectin.
- Made patients avoid seeking an ivermectin prescription from a health care provider.
- Made patients refuse a prescription for ivermectin if offerred one by a health care provider.
- Made pharmacists unwilling to fill a prescription for such a dangerous, ineffective medicine.
- Made hospital and pharmacy administrators remove the dangerous, ineffective drug from hospital formularies.
- Made health care leaders propose policies and/or legislation to disallow providers from treating patients with such a dangerous, ineffective medicine.
- Made U.S Customs willing to search for and confiscate incoming shipments of such a dangerous, ineffective medicine.
- Supported health agencies in formulating recommendations against use of such a dangerous, ineffective drug.
- Made medical boards investigate and de-license physicians who prescribed ivermectin to their patients.
Again, although many societal forces participated in censoring data and disseminating propaganda on ivermectin, none of their actions would have been defensible or possible without the supporting “science.” The problem is that the only “science” that society seems to pay attention to or be guided by is that which appears in high-impact medical journals.
Thus, if you control the high-impact journals, you control the “science.” The Pharmaceutical Industry figured this out long ago, and is a reality that has been written about extensively, often by previous high-impact journal Editors like Dr. Marcia Angell and others. Despite their efforts in exposing this truth, the implicit faith and trust in the wisdom and quality of the science in those journals has still not been shaken. Not by the media, the doctors, or the laypeople. Especially the doctors. They revere those journals and do exactly what those journals tell them to do.
Remember that the worlds highest-impact medical journals are the New England Journal of Medicine (NEJM), the Journal of the American Medical Association (JAMA), NEJM, The Lancet, the British Medical Journal (BMJ), and the Annals of Internal Medicine (Cochrane Library is the top journal of systematic reviews/meta-analyses). Although the definition of “high-impact” is a scientific one, i.e. that the papers in those journals are the most cited among all scientific manuscripts, I interpret the term differently. High-impact to me means that when a study is published in those journals, it can immediately drive news headlines. The press is alerted prior to publication of any new important study finding, whether positive or negative. Science reporters (which technically do NOT exist anymore) get to ask the study investigators questions about the study design, conduct, or conclusions and thus they can write up newsworthy headlines and articles which appear on the same day as the study’s publication. Since the world’s eyes were on ivermectin as a possible treatment, the studies appearing in those journals made big headlines. It should go without saying that the positive studies published outside the high-impact journals, no matter how large or high quality, never generated any headlines in major media outlets.
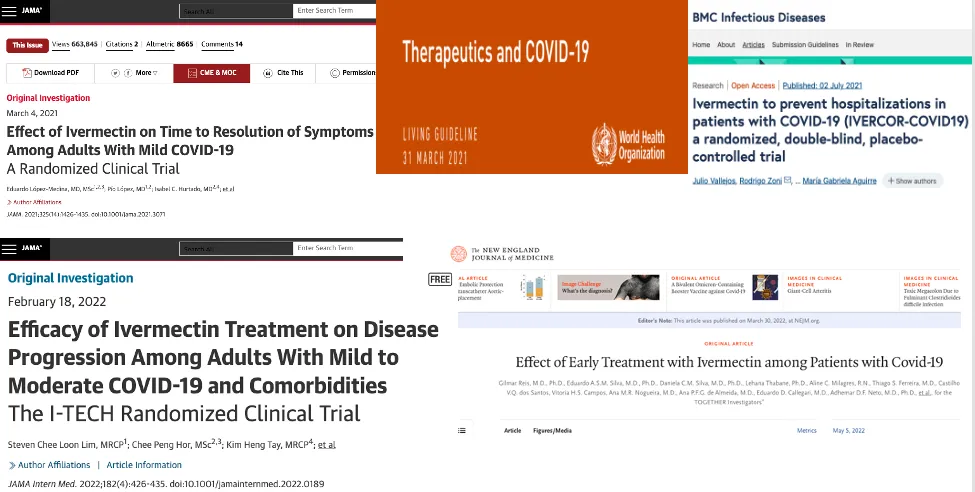
Anyway, the point of this post is to compile the fraudulent studies and meta-analyses of ivermectin that launched all the headlines supporting the Disinformation campaigns. These five are emblazoned in my memory:
I can recite the above five studies without thinking because the day each appeared on the website of their respective medical journal, I had to wake up to the FLCCC team’s numerous emails, texts, and phone calls letting me know we “had to do something” because with each publication and the media storm that ensued, the FLCCC was asked to defend our position or were condescended to as “you guys got it wrong.”
Each day was a PR crisis in terms of having to defend our credibility and treatment recommendations. I hated each and every one of those days. Hundreds of doctors arrogantly tweeting and posting “see I told you it didn’t work”, journalists writing hit jobs, calling us “advocates” or worse, “fringe anti-vaxxers” etc. It was a shit show. And it was exhausting beyond belief.
Notice the dates of publication of these trials. I point this out because it seemed to me, with my front row seat, that these studies and mass media campaigns were spaced out in timed intervals. It was like a cannon firing every few months, with each propaganda round sounding louder and traveling farther… until everyone in the world thought the same thing, “ivermectin doesn’t work.” This hypothesis might explain why the TOGETHER trial (the most fraudulent and impactful of them all) took literally 9 months to appear after the study was terminated and the preliminary results were announced in an NIH presentation. I think they held on to it in order to time its impact for whenever there was a “dry spell” of bad news against ivermectin. Pharma knows how to conduct Disinformation campaigns.
To wit:
March 2021 – Lopez Medina/JAMA.
April 2021 – WHO Guideline.
July 2021– Vallejos/BMC Infectious Disease.
February 2022 – Loon Lim/JAMA.
May 2022 – Reis, NEJM.
Now, one of the main issues with all of the high-impact journal trials that were purportedly negative, and which escaped the attention of the entire world is that… most were done in South American countries where ivermectin was not only available over the counter but its efficacy was increasingly recognized by word-of-mouth and through social media and even media and some governments.
There is abundant evidence that the control groups were not only taking ivermectin but also that the pharma-conflicted study investigators were literally taking little to no action to identify those taking ivermectin and to exclude them from participation. Which makes it very very hard to prove that ivermectin is more effective than ivermectin. With both groups getting ivermectin, this led to very few hospitalizations or deaths, and thus what is called an “underpowered trial.” By definition, when a study is underpowered, most differences between treatment groups will not reach statistical significance. Double whammy. With rare exception, these limitations were not mentioned in the manuscript and especially not the conclusion. Yet, each time they were published, the uncritical news media went wild screaming “ivermectin doesn’t work.”
Watching those trials get published, then heralded as “large, high quality, rigorous trials” celebrated across academia and media has been one of the great sadnesses of my life. Hundreds of thousands of doctors across the world who were using ivermectin and knew it was efficacious had to witness the same thing. I had to observe entire societies where ivermectin then literally became either outlawed (Australia), removed from hospital formularies (entire U.S), and/or restricted in use while case and death counts rose in massive waves (most of the world).. all as a result of counterfeit or mis-interpreted science.
Complaints about the innumerable flaws in study design and conduct fell on deaf ears, found zero media traction (shocker), or were dismissed as the whining of sore losers or some such. Yet these flawed design tactics kept re-appearing and re-appearing, as if from some sort of trial design playbook called “how to design a trial to show a lack of treatment effect.” Design flaws such as:
- Avoiding the application of strict criteria to identify and exclude subjects taking ivermectin from the control/placebo groups.
- Enrolling only mildly ill, young, or otherwise healthy patients with a primary endpoint of measuring differences in hospitalization while so few went to the hospital.
- Administering as low of a dose or for as short a duration as possible.
- Administering ivermectin on an empty stomach despite knowing concentrations are higher with a meal.
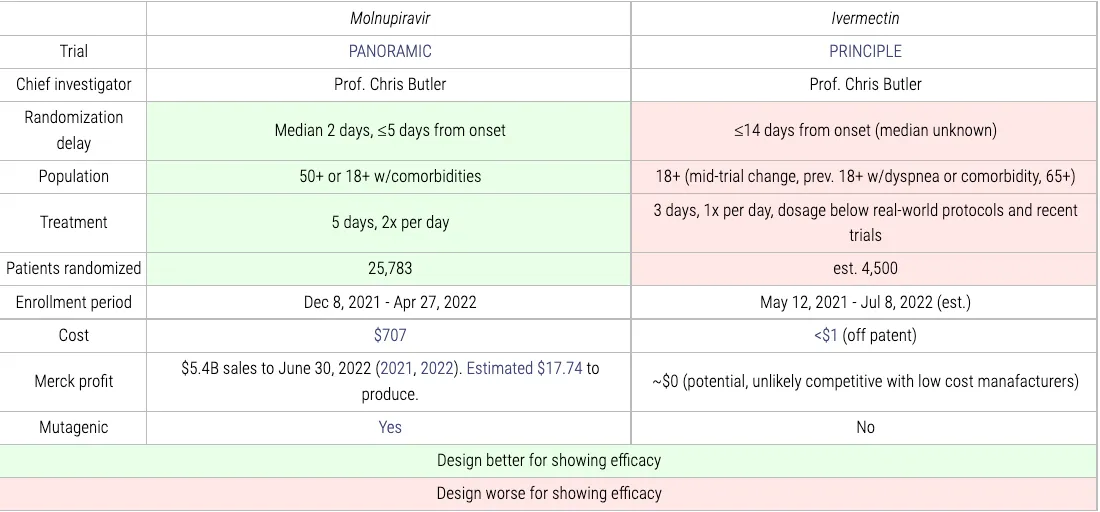
- Placing arbitrary, made-up, unprecedented weight limits to dosing such that the highest risk patients (obese) were under-dosed. To wit, the only trials with such weight limits were the ones described as “large, high-quality, rigorous” trials: ACTIV-6: 87.5kg, TOGETHER: 90kg, PRINCIPLE:100kg, COVID-OUT:157.5kg
- Enrolling patients many days into the disease, after their trajectory was already set.
- This study design feature was the opposite of what Pfizer did in their Paxlovid trial where all subjects were treated within 3 days of onset of symptoms.
- This study design feature was the opposite of what Merck did in their Molnupiravir trial where they literally enrolled 25,000 patients a median of 2 days from first symptoms. Please read that again. Meanwhile almost all of the “large, high-quality, and rigorous” ivermectin trials allowed up to 7 days to enroll in the study, and the most farcical is the Oxford PRINCIPLE trial which .. allowed enrollment up to 14 days from first symptoms. Yup. Note both trials have the same principal investigator.

Also note that the PRINCIPLE results have not been released yet, despite having completed enrollment in July of 2022. Crickets from that trial despite their beginning enrollment in the ivermectin arm in May of 2021, now nearly 18 months ago. Look at this awesome table by the superlative c19early.com group. Again, the Principal Investigator Chris Butler (I am not calling him a Professor) is the same for both trials and thus was involved in the design of both. Hey Chris, why were the study designs so different?
Insanely obvious no? My list from above were not the only tactics and flaws we identified, but they are the main and most consistent ones. Despite these repeated actions, in their papers the study authors consistently concluded, often definitively, that ivermectin had no efficacy or went further with blatantly idiotic policy-making statements such as “these findings do not support the use of ivermectin for treatment of mild COVID-19.” Pure propaganda. But only a tiny sliver of doctors read beyond the abstract conclusions. Heck only a minority of doctors read the journals. From what it looked like to me in COVID, most were learning about COVID, ivermectin, and the vaccines through the media. Pharma knows this.
Ok, lets go briefly through the trials and their ensuing media campaigns “debunking” the ivermectin “craze.” Notice how vaccines were never described as a “craze” by the media and they definitely don’t work.
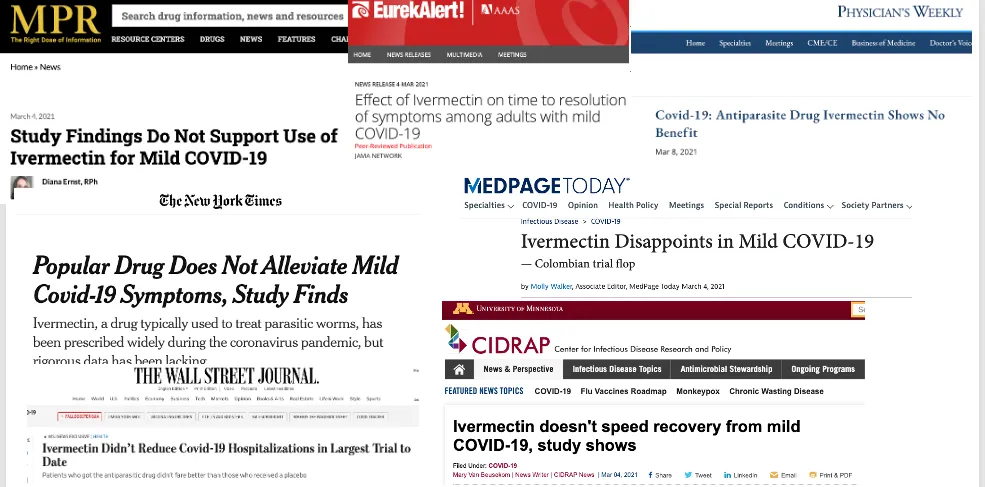
- JAMA, March 4th 2021, the “Lopez-Medina” trial:

Short take of issues:
Done by deeply Pharma-conflicted Investigators who gave ivermectin too late, on an empty stomach, in mildly ill, healthy patients with most of the control group already on ivermectin. Despite these shenanigans, the study found a lower mortality, lower disease progression, lower treatment escalation, and faster resolution of symptoms with treatment, without reaching statistical significance.
Longer take:
- One hundred doctors wrote an open letter to JAMA pointing out its almost innumerable flaws and asked for a retraction. It was ignored.
- Alexandros Marino’s “deep dive” uncovered even more fraudulent actions, see my post of his analysis of this trial.
- The c19early.com groups take, brilliant and comprehensively detailed as always. A master class really.
PR Campaign that the study launched: (notice that Pharma does not have to do anything once a trial like this is published in these journals – the PR campaign writes and conducts itself through uncritical, obsequious media). Not one criticism of the trial.
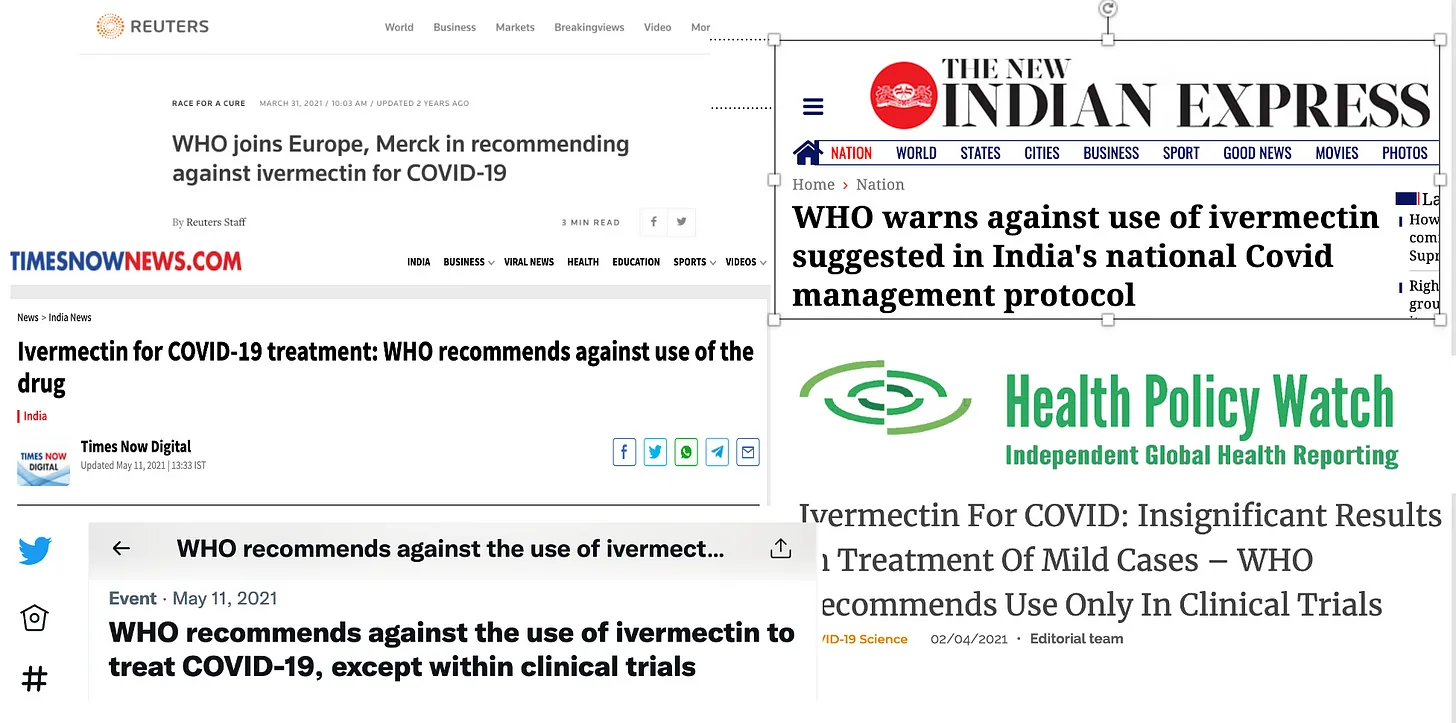
- WHO Guideline Committee meta-analysis, March 31, 2021.

My short take on the corrupt actions by the WHO:
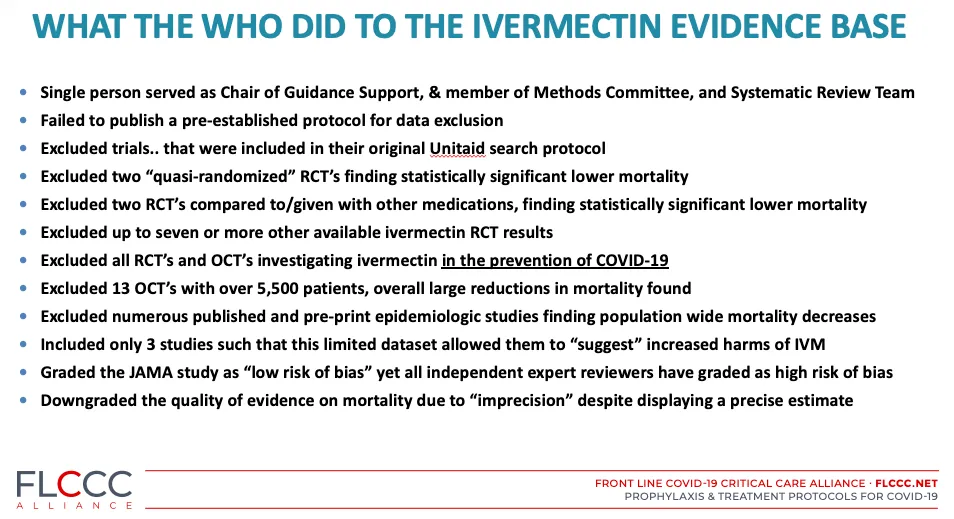
I spent weeks writing a white paper on this atrocity. Again, had the WHO instead issued a “conditional” recommendation, which the evidence at that time fully supported, the entire trajectory of the pandemic would have been altered. Public health my ass.
More negative PR against ivermectin flies around the world:
- BMC Infectious Diseases, July, 2021
Short Take: very low dose (0.15mg/kg) with only 2 days of treatment. Overall low-risk patients, only 7% hospitalized, thus trial underpowered. Literally, you cannot make this up: 74 patients had symptoms for >= 7 days. Most importantly: 55% of potential subjects were excluded for taking ivermectin within 7 days. Problem with this: those that took ivermectin prior to 7 days does not completely remove its efficacy. Whatever. Just subtle trial criteria nonsense that no-one, and I mean non-one (except for me and other ivermectin experts) pay attention to or let influence how they interpret the trials conclusions. Again, they do not have to be subtle. The only thing that matters is what the study abstract conclusions says. Get this – the trial still found a reduction in hospitalization, not statistically significant of course, thus the abstract conclusion that ivermectin doesn’t work. So tiresome.
Longer take: As usual, the obsessively detailed brilliance of the c19early.com group here.
- I-Tech Trial, Malaysia, JAMA, February 18, 2022

Short take and long take: I did a deep dive on the absurd discord between the positive, supportive data for ivermectin that were found in this trial with how it was “presented to the world” in the journal I call “PHAMA”, not JAMA. You may have read my post on this absurdity back then, but go re-read it again, here. Might make more sense now.
PR Campaign it launched: please pay particular attention to this “fact-checking” article going after John Campbell who rightly emphasized the proper way to interpret its willfully limited findings here. The most enraging article was this one here, invoking the mantra of “evidence based medicine” to disprove all the “advocates” etc. Again, exhausting and tiresome.. and deadly.
PR Campaign: note the synchronous outcries from Medpage today, WebMD and Medscape, hitting almost all U.S doctors:
Despite the near statistically significant reduction in mortality, the lead author wrote the below, even taking a personal dig at me for my unfortunate use of the term “miracle drug” in my Senate testimony (for the record I never called it a miracle drug, but rather I spoke about its “miraculous efficacy” and immediately followed that with “and I don’t want to be sensationalized by that statement.” But, you know, just facts.
“Essentially, our study findings have dismissed the notion of ivermectin being a ‘miracle drug’ against COVID-19. Individuals infected with COVID-19 should not resort to self-medication with ivermectin. Having a false sense of recovery while taking an ineffective drug could lead to delay in seeking appropriate medical care, thus resulting in poorer outcomes.”
I wish I could give him a good slap in the face. Sorry if that sounds immature but geez, I need to slap someone. Maybe I will slap Ed Mills instead, he lives closer. Remember Ed? He is the mastermind behind the most fraudulent trial of them all, a trial which sailed through peer-review to land on the front page of the highest impact journal in the world, the New England Journal of Medicine. See below.
I have written a ton about this bad boy, compiling not only my own analysis, but those of my deeply expert colleagues. My three part series on just this one trial is here, here, and here. The last one details numerous atrocious and disturbing comments uttered by the investigators of that trial. Bastards.
My analyses admittedly were written emotionally as well as scientifically. If you prefer a more “sober”, “objective” analysis, please read this review of the trial published by the Cato Institute. It is masterful, and almost looks like they re-wrote my own review but in a more “academic” fashion and tone. Check it out. They did not conclude with having a desire to slap the Principle Investigator Ed Mills but they seemed close.
The most hilarious and deeply troubling outcome of this trial was when it won the “Trial of the Year” by the Society of Clinical Trials. This celebratory article was published on Ed Mill’s company page, Cytel, a contract research organization that literally works for pharmaceutical companies to “gain approval” of their products. Good times.
The PR campaign it launched was, in my mind, the final nail in the coffin of ivermectin. Headlines are painful. One included a picture of Trump holding a mask. What?

Ok, so we covered the fraudulent “rigorous” trials that were published in the high-impact journals. In Part 2, I will cover the meta-analyses and editorials published by the same journals. In terms of brazen fraudulence, things get worse, like way worse.
I just want to say thanks to all my subscribers, especially the paid ones! Your support is greatly appreciated as it allows me to devote what is often large amounts of time I spend researching and writing my posts, so again, thanks.
P.S. I opened a tele-health clinic providing care not only in the prevention and treatment of acute COVID, but with a specialized focus on the study and treatment of both Long-Haul and Post-Vaccination injury syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.P.S We held the world’s first conference on understanding and treating Spike protein induced disease this past weekend (i.e long haul COVID and vaccine injury syndromes). All the recorded lectures will be available for download later this week on the FLCCC website. Link in my next post.

P.P.P.S. I am writing a book about what I have personally witnessed and learned during Pharma’s historic Disinformation war on ivermectin. Pre-order here for: