
And choline too
You can expect this to be somewhat good news with a lot of smugness behind it. I have been waiting for evidence on this for a very, very long time. By sheer coincidence, I was tagged in this tweet earlier Saturday.
Nicotine exposure decreases likelihood of SARS-CoV-2 RNA expression and neuropathology in the hACE2 mouse brain but not moribundity
Individuals infected by SARS-CoV-2 are at risk of developing neurological-related post-acute disorders. Disputed epidemiological data indicated nicotine may reduce the severity of infection. Here we find exposure to nicotine in drinking water does not alter the moribundity of hACE2 mice. However, pre-exposure to nicotine decreased the likelihood of SARS-CoV-2 RNA expression and pathology in the brain. These results suggest mechanisms involving targets of nicotine could be leveraged to prevent the neurovirulence of SARS-CoV-2.
Discussing nicotine will come with many caveats and for most people with those with scientific literacy is hard to go through the evidence, because this one has decades of negative bias built upon. Similar to what is observed in the abstract of the paper (above), many of the benefits of nicotine come from “chronic” exposure, somewhat of a long-term use, rather than a momentary intervention.
Early epidemiological evidence suggested nicotine usage can decrease COVID-19 severity8. These findings have been disputed9,10 as smoking is a well-defined risk factor for respiratory viral infections due to peribronchiolar inflammation and epithelial cell damage11. Still, multiple mechanistic hypotheses12,13,14 arguing for a possible therapeutic effect from nicotine have been proposed based on altered gene expression of ACE215,16,17 and immune/inflammatory responses18,19,20. The first randomized, double-blind, placebo-controlled, multicenter trial (NCT04583410) concluded nicotine patches did not reduce mortality or rates of anxiety, depression, PTSD, or insomnia eight weeks after nicotine tapering in patients requiring mechanical ventilation from COVID-19-related pneumonia21. Despite the lack of nicotine’s efficacy as a post-inoculation therapy, the possible therapeutic effects of nicotine prior to inoculation and potential impact on PASC severity still needs to be determined. In the current study, we tested the hypothesis that nicotine intake prior to SARS-CoV-2 inoculation would decrease moribundity, neural expression of SARS-CoV-2 RNA, and neuropathology in hACE2 mice.
The first highlight of this paragraph is to serve as a reference for those who want to indulge in further reading, the second I have a few problems, as I usually do with many of these “trials”. A patient that required mechanical ventilation would never benefit from nicotine alone, not even half a dozen supplements, and in regards to nicotine, 8 weeks for such cases is “too little”. I would love to see what they would find by adding nicotine, tryptophan, and niacin for 8 weeks though.
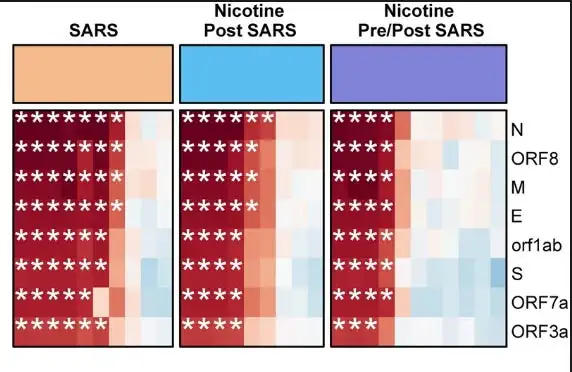
Protein expression, without nicotine, post-SARS exposure, and pre and post-SARS exposure, with the biggest benefits coming from pre and post. Regardless of nicotine exposure, ACE2 downregulation was present. In simple terms, so farm, it doesn’t affect the overall course of infection, but it does affect how much of these proteins are present, to say diminishing any potential damage, given how parts of many of these proteins are directly linked not only to damage in many organs but to Long Covid and autoimmunity, this is rather good.
Nicotine Pre/Post SARS mice were 3.15 × less likely (Fisher’s exact test, p = 0.0004) to show high SARS-CoV-2 RNA expression in brain tissue compared to SARS mice and 1.87 × less likely (Fisher’s exact test, p = 0.0015) to show high SARS-CoV-2 RNA expression in brain tissue compared to Nicotine Post SARS mice.
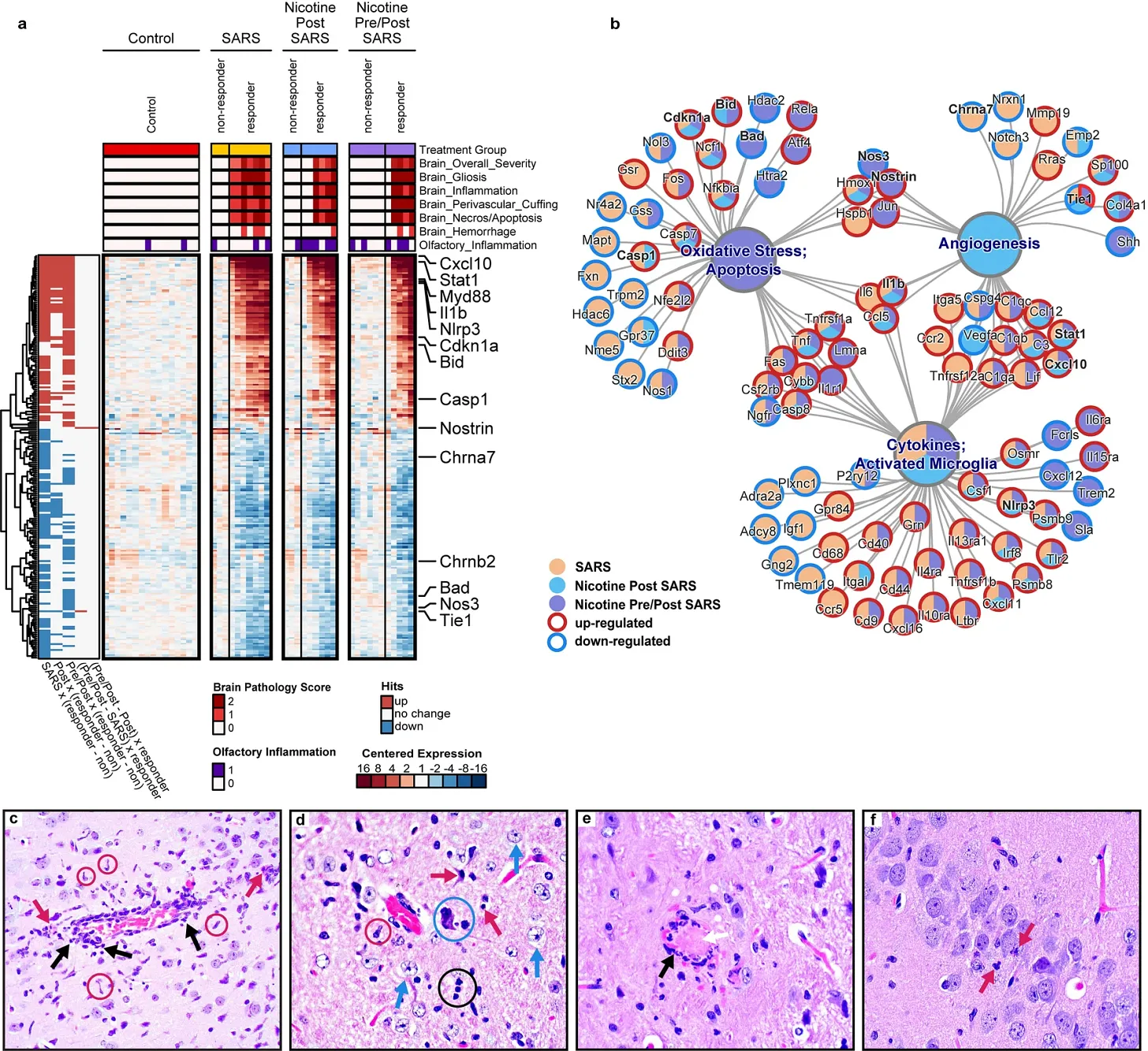
The papers go further to categorize the presence of SARS-CoV-2 RNA in the brain, both as a heatmap (image a, the more red, the higher the presence), and a pathway network nodal structure (image b), and the 4 images below microscopy images of the damage in brain tissue. (In case you ever wondered how I do what I do, the heatmap is often useful, but the image b is often the one that gives you the most answers if you know how to look at it).
Per the description of the author throughout the entire paper, the presence of SARS-CoV-2 RNA in brain tissue correlates with the presence of minimal to mild lesion, the presence of inflammation, gliosis (brain cells that causes more damage in the brain), inflammation of the blood vessels around certain regions of the brain and necrosis, entirely correlated with the RNA presence, the more viral presence in the brain, more damage is found.
Inflammatory infiltrates were comprised of mononuclear cells, macrophages, and neutrophils. Inflammation was followed by trails of degenerative/necrotic lesions and was commonly identified in the fronto-parietal cortex, piriform cortex, caudate putamen, septal nuclei, nucleus accumbens, olfactory tracts, hippocampus, habenular nuclei, thalamus, hypothalamus, amygdala, and brain stem.
As I (and many before me) proposed a couple of years ago, most of the damage is immune-mediated, and the regions that suffered damage were quite plenty. Authors go on to reaffirm that exposure to nicotine shifted the likelihood of neuroinvasion, but not the degree to which the virus invaded the brain of the mice that had RNA present in the brain.
So, how that works, and why it is so important ? Some readers might know from the first sentence alone.
The targets of nicotine, nAChRs, are ligand-gated ion channels expressed in many tissues including microglia, neurons, and the epithelium of the airway and blood–brain barrier25. nAChRs have been found to blunt the natural immune response to infection via the cholinergic anti-inflammatory pathway26. This function is critical as an altered inflammasome profile in the cerebral microvasculature is predicted to be the initiating factor leading to neuronophagia27. While we do not currently have enough information to make a conclusion, we hypothesize that chronic binding of nicotine to nAChRs on epithelial cells and microglia might desensitize the nAChRs, leading to a suppressed hyperimmune response during the SARS-related cytokine storm, maintaining blood–brain barrier integrity28,29,30,31. This hypothesis is supported by epidemiological evidence suggesting an adverse role of α7 nAChRs as expression of the negative dominate version, CHRFAM7A, is correlated with reduced COVID-19 severity32. This may be due to an α7 nAChR-mediated upregulation of ACE2 in airway epithelial cells17, as seen in regular smokers16, theoretically raising the risk of viral entry in local tissue. Although, the present study found that nicotine exposure had no detectable effect on the SARS-CoV-2-mediated reductions in ACE2 expression potentially due to the nicotine exposure method and/or cell type. While non-nicotine exposed responder mice exhibited reductions in Chrna7, those exposed to nicotine did not. It is unclear what this change in expression represents as there were no differences in histopathology or pathology-related genes between responders, regardless of nicotine exposure. Of note, in silico analyses have indicated favorable binding of the spike protein directly to α7 nAChRs12,33,34, however recent mechanistic work failed to detect a physiological interaction between the two35.
As I mentioned and asked the reader to write down a specific receptor in the “NAC and Metformin are beneficial in Long Covid”, the receptors referred to here are “family members” of the one mentioned in the aforementioned substack. In regards to SARS-CoV-2 nAChRs (nicotinic acetylcholine receptors) are incredibly important given their important role not only in cells but also systemic immune response.
Some authors argue that a mutation in a very specific part of the Spike Protein, which directly interacts with one of these nAChRs is the major responsible cause for the severe diminishing pathogenicity of the virus when Omicron first appeared. As usual, we attempt to connect certain dots here, without trying to overcomplicate and to help make sense of why nicotine exposure can be so helpful.
Study: Long-term exposure to nicotine markedly reduces kynurenic acid in rat brain–in vitro and ex vivo evidence
Effects of acute (1 mg/kg, i.p.), subchronic (10-day) and chronic (30-day) administration of nicotine in drinking water (100 microg/ml) on KYNA brain content were evaluated ex vivo. Acute treatment with nicotine (1 mg/kg i.p.) did not affect KYNA level in rat brain. The subchronic exposure to nicotine in drinking water significantly increased KYNA by 43%, while chronic exposure to nicotine resulted in a reduction in KYNA by 47%. Co-administration of mecamylamine with nicotine in drinking water for 30 days reversed the effect exerted by nicotine on KYNA concentration in the cerebral cortex. The present results provide evidence for the hypothesis of reciprocal interaction between the nicotinic cholinergic system and the kynurenine pathway in the brain.
Nicotine Attenuates Disruption of Blood–Brain Barrier Induced by Saturated-Fat Feeding in Wild-Type Mice
Nicotine moderately attenuated BBB disruption induced by chronic ingestion of high-SFA diet, but had no significant effect on neuroinflammation per se .
Nicotine exposure alters in vivo human responses to endotoxin
The alpha 7 nicotinic receptor is reportedly a key element in the cholinergic anti-inflammatory pathway. Because a prototypical ligand for this receptor is nicotine, we studied the in vivo human response to bacterial endotoxin or lipopolysaccharide (LPS) in the context of nicotine or placebo pretreatment. Twelve adult male normal subjects were studied prospectively. Six received overnight transcutaneous nicotine administration by application of a standard patch (7 mg). Six hours later, all subjects were given an intravenous dose of endotoxin (2 ng/kg) and were evaluated for an additional 24 h for circulating levels of inflammatory biomarkers, vital signs and symptoms. The nicotine subjects had elevated blood levels of the nicotine metabolite, continine, prior to and throughout the 24-h post-endotoxin exposure phase. Subjects receiving nicotine exhibited a significantly lower temperature response as well as attenuated cardiovascular responses for 2·5–6 h after LPS exposure. In addition, increased circulating interkeukin (IL)-10 and cortisol levels were also noted in nicotine subjects. These data indicate an alteration in LPS-induced systemic inflammatory responses in normal subjects exposed to transcutaneous nicotine. In this model of abbreviated inflammation, nicotine exposure attenuates the febrile response to LPS and promotes a more prominent anti-inflammatory phenotype.
Brainstem cholinergic pathways diminish cardiovascular and neuroinflammatory actions of endotoxemia in rats: Role of NFκB/α7/α4β2AChRs signaling
Highlights
•Nicotine blunts LPS-evoked hypotension and cardiac autonomic dysfunction.
•Nicotine normalized NFκB and α7-nAChR expression in brainstem of endotoxic rats.
•Nicotine effects are replicated after activation of brainstem α7 or α4β2 receptors.
•Blockade of central α7 or α4β2 receptors attenuated the favorable nicotine effects.
Many of the things mentioned above were covered both recently and for most of the existence of this substack, I have covered all these pathways and their importance in relation to both the viral infection and the Spike Protein from the injection. The major “issue” here is the need to take nicotine longer term to have the benefits described above, the defined “chronic” use, this also explained why some people I know continue to be unphased by the virus, such as my own mother, a not so healthy heavy smoker (smoking will give you Niacin, Tryptophan, and Nicotine, but it is incredibly counter-productive unless you have really good mitochondrial genetics, which incidentally she has).
But this gives us an avenue for potential and cheap treatment and intervention for both people developing sequelae from recent viral infections, and anyone within specific subsets of Long Covid. Also given the compromised naturally at multiple physiological levels of the multiple times mRNA-vaccinated, nicotine would be an incredible addition to recover from the potential damage caused by the gene therapy.
Upon careful analysis of each person, nicotine intervention would benefit many Long Covid patients, especially the ones that show any relation to endotoxin-related dysfunction, byproducts of the exposure to LPS via Spike Protein, and by default dealing with the harsher side of the Kynurenine Pathway.
Why eggs ? Eggs are a super-food, rich in many essential nutrients, but above all else, one of the best sources of Choline, which plays many essential functions, such as maintaining lung integrity, and the list goes on, but above all else, choline can be selective α7 nAChRs agonist, and also helping with inflammatory responses.
In case you were not aware, early in the pandemic, the Chinese government basically obligated everyone treated in their hospitals to take a bunch of drugs, and as primary care to eat 4 eggs a day, incidentally 4 eggs a day will give you the recommended choline you need daily.
Choline Supplementation Modifies the Effects of Developmental Alcohol Exposure on Immune Responses in Adult Rats
In contrast, in the plasma, choline reduced LPS-related increases in pro-inflammatory markers, particularly in ethanol-exposed subjects. Thus, early choline supplementation may modify both brain and peripheral inflammation. These results suggest that early choline can mitigate some long-term effects of ethanol exposure on hippocampal inflammation, which may contribute to improved hippocampal function, and could also influence peripheral immune responses that may impact overall health.
Choline supplementation is very beneficial for anyone suffering from any cognitive-related issues, regardless of source, but especially from neuroinflammation (the most common source). I myself supplement choline, it is great for people who may have a genetic predisposition to any of the diseases in the dementia class (Alzheimer’s and any of the other 23 diseases) or overall cognitive function. If you use Piracetam, you must either eat a bunch of eggs+animal protein daily, or supplement choline.
In case you are about to ask me if you should supplement nicotine, only you can decide that, I do think a small portion of people would benefit from nicotine (and choline) supplementation for at least a few months, especially anyone with inflammatory-related diseases (especially in the gut, bowels) or have persistent Long Covid that didn’t improve by large margins when using antioxidants, enzymes, etc. At the very least choline every once in a while would hugely benefit your overall long-term health.
Edit
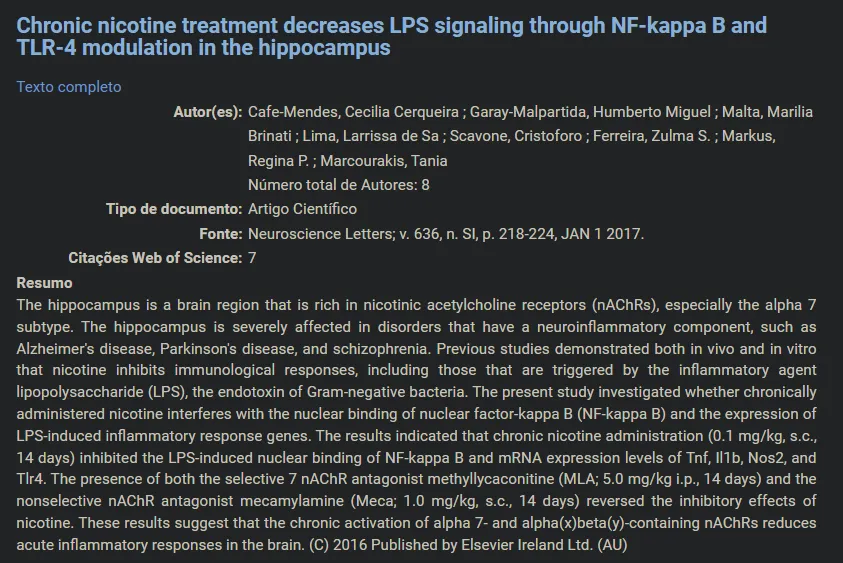
I can’t remember the last time I edited anything I published, besides correcting misspellings and some grammatical errors, but this one is different. I found the following paper today, a long time after publishing this substack. It is a great read, but the following section is the one that jumped to my eyes.
Nicotine in Inflammatory Diseases: Anti-Inflammatory and Pro-Inflammatory Effects
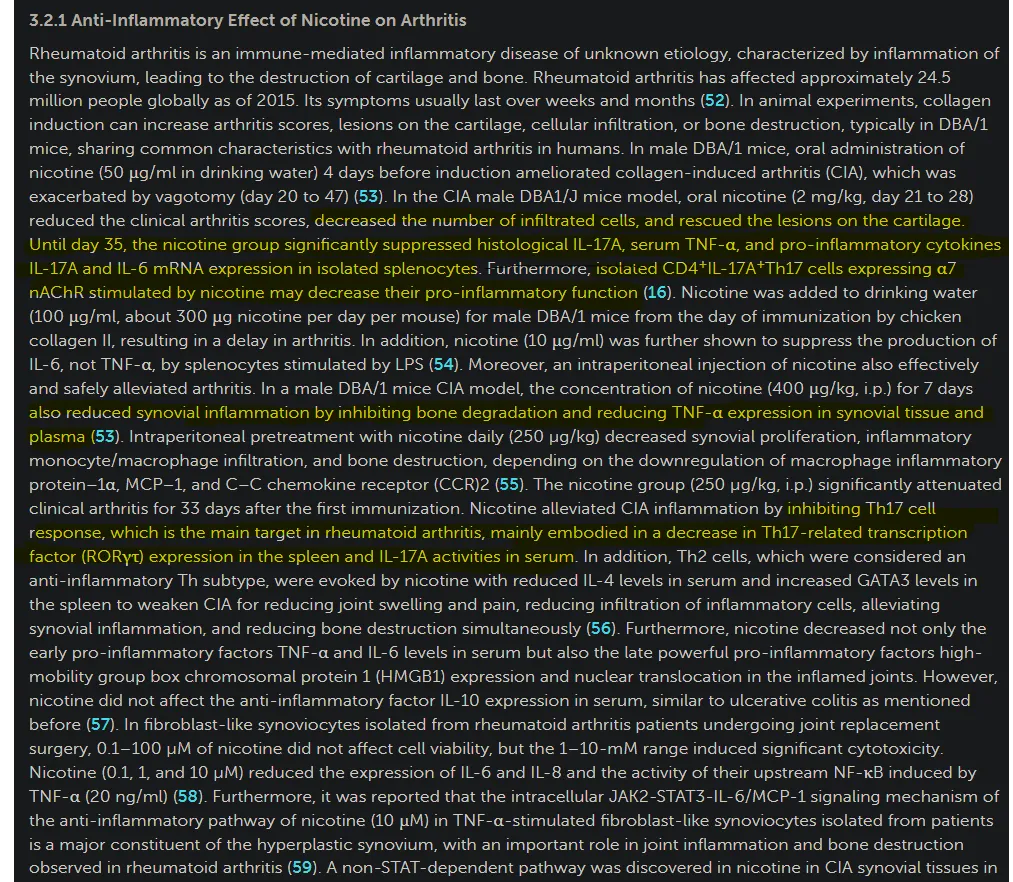
In case you are not aware, or suffering from informational deluge (when you are presented with too much information within a short period and the brain can’t process and store the information and you lose a lot of the retention) this is precisely the pathway and mechanism we first proposed as a major inducer of damage from the mRNA, and later being proved at every level of the pathway.
CD4 cells, IL17, Th17 cells, if you use any of these terms in the search function here, you will get over a dozen subtasks I wrote. Intriguing how nicotine literally diminishes the precise response the mRNA (+Spike) induces.
I am grateful for everyone who chose to support this Substack, here or on Kofi at any time, and for people who share the things they think are useful.
