
- Autopsy findings in cases of fatal COVID-19 vaccine- induced myocarditis
- VAERS myocarditis paper
- preprint autopsy paper
- Spike protein detoxification paper
- We will also cite the Nakahara paper and the Krausen paper
Transcript
0:00
you are very welcome to this video and I’m particularly pleased to welcome Dr Peter McCulla who is an internist a
0:08
cardiologist and epidemiologist he’s been a professor and a very very highly
0:13
published doctor indeed and I’m also welcoming Nick holer who is a medical
0:21
research gentleman thank you both for coming on thank
0:27
you now the basic thing we want to talk talk about today and it’s it really couldn’t be more important I’ve got so
0:34
many uh questions I want to know about this really uh but we want to look at
0:39
this paper autopsy findings postmortem findings in cases of fatal covid-19
0:45
vaccine induced myocarditis so so Dr Mulla perhaps you could just start us
0:50
off by you know telling us a little bit about what myocarditis is and and why you’re concerned about it in this
0:57
context please well myocarditis is is a is a medical problem that we’ve dealt
1:03
with in cardiology for decades as long as I can remember and uh you know prior
1:09
to covid the causes uh were kakaki virus adov virus occasionally an influenza
1:17
virus um and then an idiopathic form called giant cell myocarditis giant cell
1:23
was always the most worrisome and I’m in Dallas Texas and uh Dallas Texas LED one of the most
1:30
important clinical trials in myocarditis years ago was called the myocarditis treatment trial and there every single
1:37
patient had a biopsy done of the heart to try to diagnose uh you know exactly
1:42
what was the cause of myocarditis and what we learned from the study is that broadly applied steroids didn’t play a
1:50
role and the most lethal form was indeed this giant cell which is special histopathology giant cell in fact is so
1:56
important to diagnose that um you know we quickly moved towards transplant um and advanced circulatory support but
2:04
prior to the pandemic myocarditis occurred at a rate of you know somewhere
2:12
around four cases per million per year so in the United States that means maybe
2:19
about 1,200 cases in the entire country per year prior to the pandemic I had
2:26
only seen two in my entire practice one sadly passed away um but uh so we rarely
2:32
encountered it let me tell you something else prior to the pandemic we had guidelines written in cardiology that it
2:38
was so well known in myocarditis that exercise or The Surge of adrenaline
2:44
could be a trigger for cardiac arrest we immediately took people with myocarditis out of sports or athletic competition
2:50
that’s actually in all the guidance so we knew myocarditis if it exist uh could be fatal uh largely during two times one
2:58
during exercise and then also Al in the waking hours 3:00 a.m. to 6:00 a.m. in sleep because again there’s a surge of
3:04
adrenaline during the normal waking process MH and uh what what was it motivated you
3:10
to write this paper looking specifically at covid-19 vaccines because surely we’ve had a pandemic isn’t that going to
3:17
account for these cases of myocarditis the viral infection itself you know there was a great
3:24
concern Ralph baric published actually in the journal that I was the senior associate editor of many years American
3:30
Journal of Cardiology he published back in the 1990s that human beta Corona viruses uh
3:37
could actually cause myocarditis and animal models if actually the animals were exposed to enough of it he literally flooded the animals with beta
3:45
coronav virus could cause to myocarditis so during 2020 there was a an incredible
3:50
search for myocarditis uh there were studies in the US military the Israeli military and the
3:56
most notable one is published by Daniels and colleagues uh and was published in jamama from the Big 10 athletic league
4:03
now Nick is at the University of Michigan they’re in the Big 10 League that’s where I went to graduate school
4:09
and let me tell you what they evaluated every athlete they had 30% of the
4:14
students uh in 2020 got covid-19 so because they checked everybody and they
4:19
searched thousands of athletes to see if they developed myocarditis and we’re talking EKGs blood testing for chipon
4:27
escalating Imaging up to cardiac MRI out of thousands of uh of possibilities of
4:33
people who got sick with covid they came up with about 36 putative cases where there was some abnormality by uh by
4:41
enzymes uh troponin or by Imaging and you know what not a single hospitalization or death two Valley and
4:48
colleagues in Israel found no increase in myocarditis during 2020 above the Baseline rare cases but what happened
4:56
was a false narrative came out of the hospitalized literature where people sick enough to be hospitalized with
5:01
covid were having elevations in cardiac troponin in the ICU as would patients with pacal or hemophilus or other forms
5:09
of of pneumonia or ICU illness none of those hospitalized cases were ever
5:14
adjudicated to actually have myocarditis but it was the elevation of chonin so what came out of this was a false
5:20
talking point that was carried forward by the American College of Cardiology and the government agencies that said that Co itself causes more myocarditis
5:28
than the vaccines and nothing can be further from the truth my thinking is that with the
5:33
vaccine the amount of Spike protein produced is is unpredictable so with the
5:39
infection you’re going to get you’re going to get the virus you’re going to get a certain amount of Spike protein you’re going to develop an immune
5:44
response and that’s going to be dampened down reasonably quickly but with the vaccine who knows how much Spike protein
5:50
is going to be produced because you’re going to get systemic absorption you could get SP huge amounts of Spike
5:56
protein developing all around the body including in The myocardium is that part
6:01
of the PA pathogenesis do you think I think so Bruce Patterson at incel DX has
6:06
several per view Publications with the infection even severe cases he’s able to
6:12
find only the S1 segment of the spike protein presumably the F S2 segment is
6:18
sacrificed at the A2 receptor and it has largely receptor mediated um catabolism
6:24
but there is the S1 segment that’s found in the human body with the uh with the vaccines the messenger RNA and adov
6:30
viral DNA vaccines there’s a full length Spike protein even with the novaa it’s a full length SP Spike protein S1 and S2
6:38
that’s been demonstrated by brogna and colleagues in Germany but more importantly the quantity which you
6:43
pointed out and the only way we can really uh infer that is by the antibody Rises so the antibody Rises to the spike
6:50
protein in the natural infection are just a fraction of what we see with vaccination M Nick how did you go about
6:58
collecting the uh the data for this and the the the patients how were they selected so so we set out to search the
7:05
peer viwed literature for all the published autopsy studies that include
7:12
uh cases with covid-19 vaccines as a previous exposure um and specifically
7:17
those that that were affected by myocarditis and so we found around uh
7:23
over a thousand studies we looked through and uh we we searched through
7:29
those and in the end we came up with 28 cases um and and among these 28 cases 26
7:37
of them there only the cardiovascular system was involved in two of these
7:42
cases uh it was a consequence of multistem inflammatory syndrome um and we could talk about how
7:50
how how the mechanisms behind that how those are differentiated um I mean with
7:57
multi-stem inflammatory syndrome uh it it’s possibly due to that system
8:03
systematic circulation of Spike protein uh that that we’ve seen in a few studies
8:10
um now also one concerning finding we had was that the mean age of death was
8:17
44 years old now that that’s actually uh that’s a bit inflated because we didn’t
8:23
include uh we didn’t include the study by Gil which was two teenage boys diing
8:29
their sleep we didn’t include that study we didn’t include those ages in the descriptive statistics because they just
8:35
said teenage they didn’t say the age didn’t say so we didn’t include the uh
8:41
any estimated age estimat so if if we did if we included uh Teenage which was
8:47
probably 15 14 years old uh the mean age of death among cases would be probably
8:53
around 30 years old and that that’s really concerning because you know the these aren’t uh these aren’t 90y olds on
9:01
their deathbed with with uh five comorbidities uh so so yeah and most of
9:09
the cases died within a week of vaccination so that that established the
9:14
temporality of that so you’re careful to exclude studies where the cause of death
9:20
might have been something else you’re fairly sure that the 28 cases you’ve got were very likely to be vaccine
9:27
associated myocard itis deaths yeah that’s correct and and
9:33
actually in in in most of the cases around 18 cases uh there was the
9:40
patients had no symptoms prior to death they they just died suddenly at home uh
9:46
there was nothing suspected wrong uh they just died shortly after vaccination and and the autopsy findings
9:54
uh presented uh interesting findings that that that
10:00
no nothing else likely cause these death Dr Mulla medically how can it be that someone can be perfectly healthy one
10:07
minute no symptoms sometimes no symptoms at all and yet yet be dead a few minutes
10:12
later I mean what is going on here we have some Clues uh one there are two
10:19
prospective cohort studies that evaluated people before the vaccine and
10:24
then after one is been by man sui and colleagues from land and that was on
10:30
shot number two ages 13 to 18 and in that study it was uh roughly
10:38
2.3% actually met a a definition of myocarditis a couple of the kids were
10:44
hospitalized and then a paper by beran and colleagues from basil these were largely healthcare workers mainly mainly
10:51
female nurses on shot number three and they just evaluated tronin alone the main cardiac biomarker and they found
11:00
2.8% had uh an elevation opponent after the shot so and and there may have been
11:05
one or two cases where they would have met a a definition of myocarditis so we’re talking about 2.5% of people
11:12
actually probably do sustain some heart damage from these studies and of those
11:18
over half are completely asymptomatic from a cardiac perspective so and there were two papers by Jenna shower in the
11:24
journal Pediatrics that caught my attention she was uh recording children who develop myocarditis and a large
11:31
fraction had no specific cardiac symptoms they had a sore arm they had fever but nothing that would localize to
11:38
the heart and in uh our paper uh that you know I published with Nick huler at the University of Michigan uh what we
11:44
found is that no one had an MRI ahead of time to diagnose this ahead of time so
11:51
these cases turned out to be you know largely cardiac arrest and then the then the finding of myocarditis at autopsy
11:57
mhm do you think it’s possible possible that you could have two patients with the same degree of postvaccine
12:03
myocarditis and one takes it easy and maybe does a bit of academic work for a few days but one decides to play a game
12:09
of football or go for a run and because of the exercise it’s quite possible that
12:14
one could go into like something like a ventricular fibrillation cardiac arrest and the other might as it were get away
12:21
with it is is is that element of Ju Just sheer probability and bad luck in that
12:27
do you think sometimes it it changes the probabilities remember exercise is the surge of adrenaline exercise shifts
12:34
there there’s one paper from Thailand that caught my attention by IDT and colleagues that found that polymorphisms
12:42
in the scn5a sodium Channel were associated
12:47
with cardiac arrest in the setting of vaccine M genetic variability really yes so there could be genetic variability
12:54
and also uh papers that we find that the myocarditis is very patchy uh it’s not
13:01
very extensive uh it’s typically not enough to cause heart failure just as a general uh rule it would take about 15%
13:10
of The myocardium that we would see on MRI by late gum enhancement or would see by histopathology 15% of left ventricle
13:17
before there would be left ventricular dysfunction in autopsies that we had reviewed there was small patches of
13:23
inflammation but here’s the concept as The myocardium is depolarized ing if the
13:31
the wavefront of depolarization goes through an area where there is inflammation and edema there is slowed
13:38
conduction and an opportunity for that wavefront to Circle back and then cause
13:43
re-entry and when there’s re-entry that is the most common mechanism for
13:49
ventricular teoc cardia and in a young person the ventricular techic cardia is going to be fast many times it’s going
13:56
to cause a prein Sy snable uh symptoms and then will quickly degenerate to
14:02
ventricular fibrillation because the VT so fast and that looks to me like what we’re seeing on these athletes
14:08
particularly those in Europe who die on the pitch and I suppose if you had an area of uh inflammation in the
14:15
ventricular myocardium as well that itself could be a possible source of ectopic poai it can it can be ectopic F
14:22
but it’s it’s unlikely to be primary VF the most likely mechanism is initially
14:28
ventricular attack of cardia with rapid degradation to ventricular fibrillation and recently we’ve been made aware of a
14:35
paper from Japan were exactly they caught that there so there was a young Japanese man uh the first author of this
14:43
paper is um uh uh manato and a young man is on the
14:51
SEC SEC day after he takes fizer he gets a fever he collapses and the paramedics uh retreat
14:58
him and he’s in a fast ventricular tardia degenerates the ventricular fibrillations they’ve actually caught
15:04
the entire episode now uh another factor to consider in these fatal cases like
15:10
the manado case and another Case by Choy is involvement of the conduction system
15:16
so if the inflammation involves the conduction system we’re talking the AV node the bundle of His the right and
15:22
left bundle then it’s far more likely to be fatal Choy basically you know
15:27
recorded a who who literally died 7 hours into the hospital and when they did the autopsy the entire conduction
15:34
system was destroyed with vaccine induc my carditis wow incredible yeah um now
15:41
staggering I’m reading in this paper about 70% of the world’s population have had uh one at least one
15:49
covid vaccine and look looking back the incredulity is just huge that this could
15:54
be done without proper cardiac uh studies a lot of people in my comments
16:00
are really concerned that there’s an epidemic of heart failure and other heart pathologist but probably
16:05
particularly heart failure or increased cardiac arrests or increased coronary
16:10
arterial atherosclerosis uh coming um is the are
16:17
these fears in any way Justified I think they are but but but
16:23
covid the respiratory illness and the vaccines need to be factored in and and
16:28
important citations one is by X and colleagues from the US Veterans Administration clearly demonstrating
16:36
after covid respiratory illness there’s about a six- week period where older
16:42
individuals are at increased risk for myocardial infarction stroke and cardiovascular death so it’s a post
16:48
viral risk probably related to you know ethos scerotic inflammation by the way
16:54
very similar pattern after influenza same type of pattern so it’s it’s true
16:59
now with the vaccines we’re seeing this pattern of these vaccines uh and then
17:05
Cardiac Arrest uh the vaccines there’s about 800 papers in the peerreview
17:10
literature you know implicating the vaccines with myocarditis our agencies came out pretty quickly uh in 2021 and
17:18
said the vaccines caused myocarditis us FDA did I know believe it or not in the UK and Australia they came out pretty
17:25
quickly with guidelines on how to diagnose vaccine and mtis what’s incredible what’s really incredible
17:32
though is is after our agencies told us that the vaccines cause
17:38
myocarditis and we know with myocarditis athletes cannot exercise then the athletic leagues many
17:45
of them including the US NFL and others they mandated the vaccines with no
17:50
safety it’s interesting so during covid the respiratory illness there was lots of safety there was myocarditis
17:56
screening programs going on nobody could find you know basically any significant cases but when the vaccines come out and
18:03
the agencies say they cause myocarditis then suddenly there’s no safety screening or any other you know measures
18:10
the athletes take the vaccine and then we see what happens and it’s quite possible that many of these cardiac
18:16
arrests that have been so well publicized are caused by this and if these people had been advised that there
18:21
was an element of risk here and to rest for a period of time after the vaccine
18:26
it’s not inconceivable that these death could have been prevented that’s true but I tell you the
18:32
case that comes to my attention is Oscar Cabrera adamus adamus is a Dominican
18:37
player he’s playing in the the Spanish leagues doesn’t want to take the vaccines he tweets this out he’s forced
18:44
to take it in 2021 he has a cardiac arrest on the court it’s it’s filmed he
18:50
gets CPR he gets defibrillation he survives he appropriately you know is
18:55
taken out of competition he’s you know supposedly treated apparently treated and he’s trying to return to competition
19:02
and it’s now 2 years later in 2023 and he dies on a medical stress test dies on
19:08
AIC and I supervise stress tests as a cardiologist I’ve never had a death I mean we’ve had VT we even had VF but we
19:14
can always shock and resuscitate and so the adamus case of myocarditis from the
19:20
vaccine in 2021 in cardiac arrest in 2023 does give us great concern that uh
19:27
there could be inflam or scar formation and then this stochastic risk later on in life of cardiac arrest mhm so if the
19:36
vaccine had caused some physical scarring in the heart and we know that the myocytes don’t efficiently
19:42
regenerate that scarring could be there forever and could cause problems uh years or even decades down the line it
19:49
could and you know it may not be deductible by amri or even autopsy because they can be very small patches
19:56
and then we also have this uh report that’s so interesting by nakahara and colleagues regarding abnormalities in
20:03
card cardiac positron emission tomography there are about 700 vaccinated 300 unvaccinated getting pet
20:11
scans for other reasons but they had very good cardiac imaging and it was striking where virtually every vaccinated person uh The myocardium
20:19
shifted from preferring free fatty acids to preferring glucose as a metabolic substrate uh and it’s tagged with 18
20:25
floral dioxid glucose now when I order a cardiac pet and practice I’m looking for an es schic zone of myocardium here the
20:33
entire left ventricle actually took on in almost every vaccinated person the appearance of an esic left ventricle
20:40
whereas those unvaccinated had normal pet scans no fdg uptake and I looked at
20:46
the paper carefully and the only thing that makes sense to me Dr Campbell is that there may be microthrombi or just
20:53
you know RBC uh hemaglutination which is well described with the spike protein
20:58
and in the small capillaries of the heart to create these metabolic changes so I and this was seen even out to 6
21:05
months after the vaccine so we have to posit that it may not be all myocarditis it may be a form of a metabolic
21:11
cardiomyopathy or other abnormalities but it appears to be common and and we may just be seeing the
21:18
tip of the iceberg MH now most of the deaths in this study I believe occurred
21:24
3 to six days I think three days was the the medium and six days was the mean was
21:30
that right Nick the deaths was shortly after uh yeah three was the median six 6.2 I
21:38
believe was yeah okay so does that mean that the rate of deaths is going to go down quite dramatically as As Time
21:45
increases from from the vaccine in terms of these sudden cardiac
21:52
deaths yeah we don’t know Dr Campbell it may be selection bias meaning the dust that occurred Rel relatively close to
21:58
the vaccine it came to the attention of the family and the medical examiners and that you know a death that occurred 6 or
22:05
N9 months later no one may connect it and it actually may not come to autopsy
22:10
yeah yeah now one of the things I found really convincing about this paper was the uh the microscopy so here we have
22:19
evidence of uh the spike protein in cardiac tissue uh Dr Mulla what are we
22:25
looking at here please and what are these red blotches but the you know these are um basically uh
22:32
histopathologic sections of The myocardium now this is from a paper by from Germany by B and colleagues now
22:39
these are young people with myocarditis in German hospitals who are actually surviving myocarditis here these are
22:45
survivors but we use this uh image to show you the red staining is actually
22:51
the spike protein and uh now in a recent paper by crosson and colleagues they’ve
22:57
also demonstrated ated messenger RNA in The myocardium by uh a genetic uh
23:03
identification technique so I anticipate that there’s messenger RNA right in The myocardium producing the spike protein
23:11
right there and we’re seeing these red stains as a result and what do we know about these patients previous medical
23:17
history I mean do we know if they’ve had Co is there a differential diagnosis here between CID infection and vaccine
23:24
induced Spike protein uh in our uh there was actually none none tested
23:32
positive for the covid-19 virus uh at least at the time of death so we can so
23:38
the balance of probability is that this protein is is vaccine induced yeah
23:44
yeah yep and the the the blue there that they’re all cardiac muscle cells Dr M
23:50
that’s cardiac muscle cells and there’s one more paper to quote I want to make sure this is um there is a paper
23:58
of covid deaths where people have died of covid and they had an
24:04
autopsy and of Interest the hearts were examined in covid deaths not a single
24:10
case of myocarditis or evidence of myocarditis with Co alone so I think this is pretty
24:17
important we can get you the citation on this so uh this is these are interesting observations it appears as if covid-19
24:24
illness SARS kov to infection actually doesn’t cause serious myocarditis despite all the concerns in 2020 but the
24:31
big threat is covid-19 vaccination mhm and also um the these are just the
24:39
uh the blown up views of those pictures um but um also the uh inflammatory
24:46
cardiomyopathy the inflammation of the heart muscle is shown here with CD4
24:52
which are uh T helper cells um so I’m assuming that the blue here again are
24:59
the cardiac myocytes the the heart muscle and the red here is this the
25:04
staining of the uh lymphocytes the the T helper cells right the red and actually
25:11
the little dark dots now um oh yeah the dark dots that are not you know clearly
25:16
nuclei of the cardiomyocytes these are inflammatory cells uh now the important Point here is is don’t forget CD4 you
25:23
mentioned T helper cells that they they are actually in the business of trying to present antigens to B cells
25:32
and then B cells transform to plasma cells and produce antibodies so these
25:38
this is a natural inflammatory response to a foreign protein in the heart the
25:43
foreign protein is the spike protein inflammation in the heart should not
25:49
occur and anytime there’s inflammation there is an opportunity for heterogen
25:55
heterogeneous conduction through this Zone and anytime we have that there’s a risk for arhythmia I think there’s a
26:01
much bigger risk of arhythmia than there is for heart failure I’ve only had in my practice I’ve only seen two cases of
26:09
vaccine induced heart failure one man previously had heart failure he had an
26:14
icdn prior bypass surgery he took one dose of fiser and he went into cardiogenic shock and within 8 hours was
26:21
on um mechanical ventilator um ECMO support needed a heart transplant it was a very clear-cut case and then recently
26:28
I saw a case where a man took a total of three shots and after the third shot he went into hard fail with a low ejection
26:35
fraction uh and has probably missed myocarditis but uh most of what I’m seeing in the literature is just like
26:42
this the these are boys with chest pain no heart failure but they’re at risk for cardiac arrest so I suppose we should be
26:48
grateful that it’s affecting small areas of The myocardium rather than large areas of The myocardium but you’ve
26:53
already pointed out the severe risks Associated even with very small areas of The myocardium now some some
27:00
cardiologists think that the vaccine can induce inflammation in the coronary
27:07
arteries accelerating the furring up of these arteries accelerating the development of the coronary arterial
27:14
atherosclerosis what’s your thinking on that please I published a paper from our
27:20
group in Dallas Zang was the first author and we think the culprit there is the spike protein the spike protein
27:26
clearly injures endothel cells it clearly causes hemog glutation recent
27:31
paper from David shime former NIH researcher has shown that unequivocally
27:36
and that it actually induces thrombosis so I think the spike protein uh is
27:42
playing a role in episodic aosc orotic events in people with atherosclerosis uh as well as uh es
27:49
schic stroke and other atic events do you think it could actually increase the
27:54
deposition of aoma or is it more the BL clotting associated with the aoma no I
28:00
think plaque rupture is clearly in play the Zang paper suggested that and the
28:06
other issue regarding the endothelial damage and these episodic events it’s my clinical impression that the risks are
28:13
relatively equal for covid infection and the
28:18
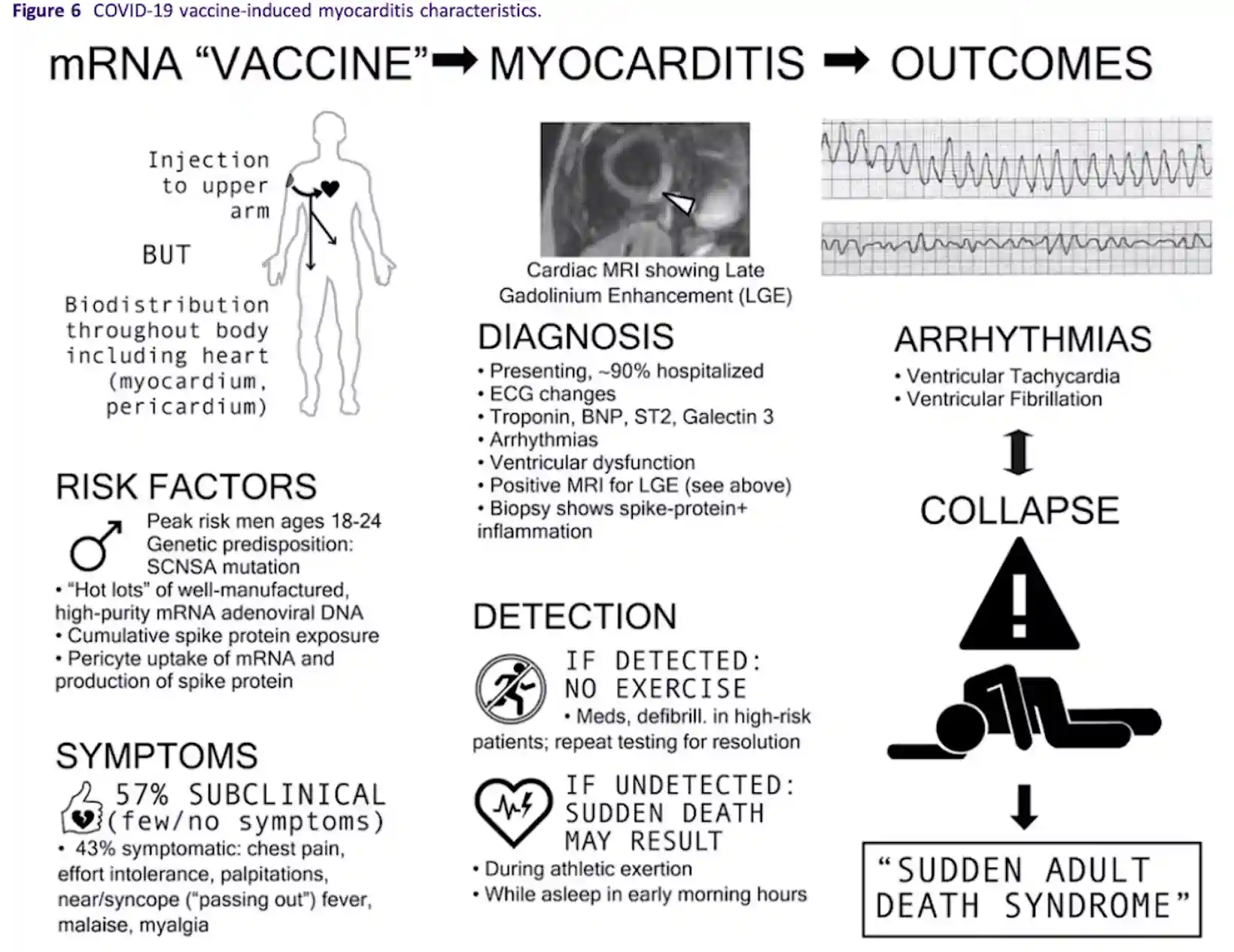
vaccine now we’ve got some sort of uh there’s a model here that you’ve basically uh sketched out which I did
28:26
find remarkably useful do you want to sort of just um tell us what the main
28:31
parts of this model are please Dr Mulla we tried to piece this together clinically what’s going on so we start
28:37
in the upper leftand corner and say listen people take an injection it’s now known that there’s biodistribution
28:43
throughout the body Crossing and colleagues showing messenger RNA in
28:48
human myocardium B the slides we reviewed shows Spike protein from the messeng RNA is physically in the heart
28:56
so there’s I don’t think there’s any debate here that the vaccine does go to the heart Spike protein is produced the
29:02
heart may actually preferentially take up messeng RNA because myocardial blood flow increases during exertion and this
29:10
may preferentially affect athletes myocardial blood flow can increase roughly two to four times with exertion
29:17
people working out M um the risk factors for myocarditis are interesting it’s
29:22
it’s men uh Peak ages 18 to 94 90% of cases are men and that was true before
29:29
covid and the pandemic myocarditis is always much higher in men than women uh
29:35
boys greater than girls and it must be related in some way to Androgen you know receptors or other factors no one
29:42
actually knows the genetic predisposition I put this down there the scn5a
29:47
mutation um uh has been described by ITT hot Lots meaning some lots have a much
29:54
greater uh risk of serious Adverse Events that’s been described by schmelling and colleagues cumulative
30:00
Spike protein exposure may play a role there’s enough cases now where people develop it on the third fourth fifth
30:07
even sixth shot there’s a fatal case of an older man recently on the sixth shot parisite uptake of messenger RNA has
30:13
been demonstrated by avolio in colleagues the symptoms are about over
30:19
half according to the two papers I quoted have few or no symptoms so they actually don’t know that they’re having
30:25
heart damage 43% symptomatic with chest pain effort intolerance palpitations near Syncopy passing out fever malays
30:33
those come to attention uh there’s our diagnosis down the middle we if they’re hospitalized EKG you know I measure
30:40
chonin BMP st2 gtin 3 those are are markers since 2013 those are our markers
30:45
in the ACC ha guidelines we monitor for cardiac arhythmia standard of care image for LV dysfunction by Echo and then
30:52
cardiac MRI and then when we see a large area in this case a large area of Lake gatal linium enhancement look where it
30:59
is Dr Campbell it’s in typically the lateral wall and the outer part of the
31:04
lateral wall almost every time it’s interesting and it’s contiguous with the parac cardium so probably the best term
31:11
to use is a myopericarditis in almost all these cases the pericardium is
31:17
involved uh if we detect it there should be no exercise we have medications for
31:23
LV dysfunction a standard of care in my practice now is we have found in the Japanese have reported this good use of
31:30
cortical steroids so we use predisone over the course of 3 months culine mandatory for a year non-steroidal
31:38
anti-inflammatories additionally for pain if there’s leano dysfunction we use evidence-based beta blockers ACE
31:44
inhibitors and the appropriate drugs large areas of Lake gatum enhancement like this one shown on MRI more than 15%
31:51
of The ventricle may need an ICD because otherwise what will happen is up top
31:57
there is the rapid ventricular tacac cardia and what you’re seeing at the top or right is VT that’s rapid enough that
32:04
would cause someone to pass out on the plane field and if not properly defibrillated it generates to the Rhythm
32:09
below that ventricular fibrillation next is a syy and that’s what we’re terming
32:15
sudden adult death syndrome you know we do think this could explain the large
32:20
number of deaths in people after vaccination with no other explanation but clinically when someone
32:27
went into that ventricular tachic cardia on the top they would faint yes and they would remain unconscious while they went
32:34
into this ventricular fibrillation that would become finer and finer until eventually we just had a AN asystolic
32:40
line and no possibility of uh resuscitation at that stage right but if you notice the fainting notice some of
32:46
the athletes particularly you can see this in the uh soccer players you call them football players the soccer players
32:52
in Europe when you get to you can see their body when they do hit the turf they’re Ty typically is some convulsive
32:58
action you’ll see some legs convulsive action a little bit that’s actually ventricular tacac cardio there is a
33:03
little bit of profusion to the brain the brain is getting enoic and then once it’s ventricular fibrillation it’s
33:09
they’re completely flaccid mhm and do we know that if this form of ventricular
33:15
fibrillation and ventricular tardia is this as amable to defibrillation as say
33:21
myocardial infarction induced VT or or VF there’s a paper by po creus as first
33:29
author I’m senior author where we we analyze this from the best we could detect in in about a thousand European
33:36
athletes and the answer is yes it’s amenable to defibrillation uh in our analysis about 40 cases could actually
33:42
be resuscitated on the field and this is with without paramedics being there there’s coaches and other people so if
33:48
we get the defibrator pads on this can be uh defibrillated um I’ve interviewed
33:54
personally and examined pilot snow in the United States he had a vaccine related Cardiac Arrest about 2 months
34:00
after taking the Jansen vaccine cardiac arrest in Dallas Fort Worth airport and
34:06
uh fortunately the miracle of his case is they called 911 and the paramedics happened to be at the gate next door
34:12
just by chance so they ran over to the jetway and it took three efforts at
34:17
defibrillation but he was defibrillated he was in VF and uh he came back no
34:22
neurologic damage he has an ICD in uh and he survived vaccine induced Cardiac
34:28
Arrest mhh now a lot of people have asked me they say well if someone
34:34
collapses if someone goes into one of these abnormal rhythms it’s very obvious
34:40
there’s a problem with the heart and we’ve started looking at the heart but do you think it’s possible because of the systemic distribution of the vaccine
34:48
and therefore the systemic distribution of the spike protein there could be similar other inflammatory processes
34:54
going on in other parts of the body as well well as the heart it’s just that we haven’t picked them up yet thinking
34:59
maybe particularly about the uh the liver perhaps the kidneys and and of course the ovaries intestines of of a
35:05
lot of concern yeah I’ll let Nick answer that because we have a larger study uh
35:10
this is the myocarditis substat of a larger autopsy study Nick do you want to take that on about kind of multi-organ
35:17
system involvement sure sure yeah so so the
35:23
other paper we or the other study we conducted um still hasn’t been published it’s on the
35:29
pre-print server of zenodo but in that paper we actually looked at all the
35:36
autopsy case studies or case series uh that include covid-19 vaccines as a
35:43
previous exposure and so in in that study we actually found yes the
35:49
cardiovascular system was was the most frequently implicated among the cases
35:54
among the 325 autopsy cases that were included uh but that was followed by
36:00
hematological System cases respiratory system and multi-stem involvement um so
36:07
so so in that study uh it was kind of 50% or so was cardiovascular but the
36:14
rest was was distributed uh throughout the body um
36:20
now um Dr MAA you want to talk about the mechanisms behind any possible
36:27
hematological right so the the hematological Fatal syndromes that are in the the larger studies on the
36:33
European commission’s anoto server uh include uh fatal uh pulmonary embolism
36:39
Veno Venus thrombo embolism I think people would accept that but also vaccine induced thrombocytopenic thr uh
36:47
pereria in in in other words the the platelets aren’t working the blood doesn’t clot properly and you kind of
36:53
get bruises all over the place as a result of that yeah well you know interesting it happened largely with the
36:58
adenoviral vaccines astroica and Jansen so there’s actually abnormal clotting and bleeding at the same time the final
37:05
mechanism of death in those cases is typically intracranial hemorrhage and thrombosis but I suppose if someone’s
37:12
blood was clotting it would be using up the clotting factors and the blood would be having difficulty to clot after that
37:17
a bit bit like a sepsis really perhaps right right and U you know one of the things that we found in both studies
37:23
that was necessary is we we actually extract all of the autopsy data into evidence tables and then we had to
37:31
independently re review it with u you know experts who in cardiac pathology
37:37
for the following reasons Dr Campbell at the time the papers were published some
37:43
of these known mechan some of these mechanisms we know now they weren’t known back then so you know some of the
37:49
earliest autopsies were done in Germany so a patient would take a vaccine and die of a pulmon embolism and and the
37:56
conclusion at the time is well it wasn’t related to the vaccine because they simply didn’t know didn’t yeah yeah but
38:02
so we know now so this this idea I think this is going to be true for a long time that that we really you can’t just read
38:09
the conclusions of the authors we have to independently review the information ourselves with contemporary
38:15
understanding well the the review process yeah we we had a fair review process three reviewers we had a method
38:22
for tie Breakers uh we did everything the right way so you know it this idea when we do a review like this we want to
38:29
make sure there’s no bias so in selection of the papers we followed you know standard uh methods Prisma search
38:36
sessions Nick produced a Prisma flow diagram and then on the adjudication and
38:42
review we we followed again standard methods to make sure it was it was rigorous now in the overall autopsy
38:48
study we found that 73.9% of cases the vaccine was either
38:54
directly the cause of death or significantly contributed to death in
38:59
the myocarditis paper that we’re reviewing um that’s fully published it was all the cases were due to the
39:06
vaccine because you know they were they were um a priority thought to be cardiac
39:11
myocarditis MH this graphic here that’s showing that uh most of the Fatal events
39:18
occurred 3 days after the vaccine going up to 36 days after the vaccine um does
39:25
this mean that people that were vaccinated a year ago can pretty well relax about
39:30
this we simp we simply don’t know Dr Campbell this is just you know the days after the
39:37
vaccine where the autopsies were performed you know in United States medical examiners don’t order autopsies
39:44
on all unexplained deaths it’s it’s really a judgment call and I think here the proximity to the the vaccine is
39:50
what’s driving this mhmh so so ni Nick you use you use something called The Bradford Hill
39:56
criteria and adjudication by expert cardiologists um because all the people
40:02
watching this or a lot of people are going to say look this is a correlation it doesn’t equal causality how do we
40:08
move from correlation to causality in in this study right well well so the Bradford
40:15
Hill criteria includes a few different categories includes strength consistency
40:21
specificity temporality so so we’ll start with we’ll start with strength of
40:27
the evidence so I mean the evidence is pretty strong we we have biopsies
40:32
autopsies that are showing uh Spike protein directly within the affected tissues uh and there’s there’s hundreds
40:40
and hundreds of studies that support the idea that that vaccines can cause
40:46
certain syndromes such as myocarditis so so I mean there’s a really large amount of strength to to the association and
40:54
the consistency scene well there’s a high really high degree of consistency um yeah there there 28 cases of fatal
41:02
myocarditis that that we found but um overall there’s thousands if not tens of
41:09
thousands of cases of myocarditis from the vaccine um so and every study has the
41:17
same findings over and over again consistency so that’s important
41:22
specificity um yeah it’s very specific uh we found Spike protein uh inside the
41:29
cardiomyocytes and those with with covid-19 vaccine induced myocarditis um
41:35
temporality as this this graphic here shows um there’s a very strong temporal
41:41
correlation between the covid-19 vaccines U and death from myocarditis um
41:49
I mean especially since the mean age of death was around Le less than a
41:54
week um and and biological plausibility again that goes back into you know is it
42:01
plausible is this C can the covid-19 vaccines is there a mechanism that can
42:07
cause the death and uh we talked about that earlier there there’s many many
42:12
different possible reasons that could contribute to death and
42:18
coherence is the is the data coherent uh you know are there major differences
42:25
between these uh you know does it make sense and yes
42:30
yes um we see very consistent findings uh with with each case um and that was
42:38
outlined um that’s what we looked at previously so all in all um The Bradford
42:46
Hill criteria seems to have met the criteria for causality for covid-19
42:52
vaccines contributing to death uh um but uh we can’t we can’t 100% say yeah
43:01
there’s a causal link um we just can’t say that as researchers until we have a
43:08
massive amount of evidence but we we can say there’s a there’s a very high likel
43:14
Dr McCulla would it be inappropriate to speculate the proportion of the excess debts that we’re currently suffering
43:19
from at the moment are attributable to this or is completely unreasonable
43:24
question we need a lot more studies you know I think what’s really needed which would be very helpful for temporal
43:30
Association is I think all countries should merge the vaccine Administration
43:36
data and the death data and you know a lot of countries have this it’s simply merging and if we saw spikes uh
43:44
temporally associated with when when people took the vaccines we could we could zero in on these deaths Dr kemell
43:50
you know in the United States our CDC V system indicates that we’ve had about 18,000 th000
43:57
Americans uh who have died and people report them to vars I’ve made these reports as a doctor I made a vars report
44:03
today um so I’m very familiar on how to do it 18,000 where we think the vaccine
44:09
caused the death okay so it’s so this is highly selected for we we think causality is there do you know of those
44:16
18,000 plus do you know 1150 occurred on the same day they took the shot sometime
44:23
right in the vaccine Center and then another 1 1200 is the next day afterwards so even if we draw a very
44:31
close time stamp here we’re looking at 30 days here I can tell you if this was
44:36
a drug trial and I was chairing the data safety monitor board which I’ve done about two dozen times in my career we
44:43
would say listen anything within 30 days any event is attributed to the
44:48
experimental product period it’s just a regulatory
44:53
standard and yet strange that this isn’t been done um I
44:59
don’t should we make a comment on why this isn’t being done have we any ideas why this data is not being taken up and
45:06
waved strongly by governments and Regulatory bodies around the world or do you want to pass on that one it’s
45:14
impossible to sign assign motive but none of the Regulatory Agencies have done a detailed evaluation of death
45:21
after the vaccine there’s been no investigation uh by any Yeah country
45:28
clearly we’re calling for that now I mean this this should be done as a matter of urgency gentlemen thank you very much
45:35
for that fascinating Insight we’ll publish this with all the links um I’m afraid I can’t guarantee how this will
45:41
be accepted by uh various uh video platforms but uh the attempt will be a
45:47
noble one so uh for your time and and all the huge amount of work and and and what you’re doing generally in promoting
45:56
health and well-being and bringing to light things that otherwise will be hidden uh on on behalf of many many
46:02
people thank you for what you’re doing thank you thank you for having us