
The public deserves a complete and transparent accounting of the Centers for Disease Control and Prevention’s safety monitoring, including the results of all interim reports and analyses, whether through an Freedom of Information Act request, Congressional order or some other means.
Summary:
- There is a disproportionately large number of adverse events reported to the Vaccine Adverse Event Reporting System (VAERS) from COVID-19 vaccines compared with other vaccines.
- There are 91x the number of deaths and 276x the number of coagulopathy events reported after COVID-19 vaccination than after flu vaccination.
- Safety signals were found for 242 adverse events using the Centers for Disease Control and Prevention’s (CDC) methodology.
- Full transparency of CDC and U.S. Food and Drug Administration (FDA) safety monitoring is urgently needed.
On Aug. 30, the CDC Advisory Committee on Immunization Practices (ACIP) voted to recommend Pfizer/BioNTech’s mRNA COVID-19 vaccine for people 16 years and older.
In comments I submitted to the committee along with my collaborators, we provided evidence of large safety signals from VAERS, using published CDC methods to analyze the data.
In this article, I describe the safety signals highlighted in our comments, which raise pressing questions about the CDC’s and FDA’s COVID vaccine safety monitoring efforts.
To begin with, there has been an unprecedented increase in the number of adverse event reports to VAERS associated with COVID-19 vaccines. The chart below shows the number of deaths for all other vaccines reported to VAERS annually since the system’s inception in 1990, compared to deaths reported for COVID-19 vaccines, from both domestic and foreign sources.
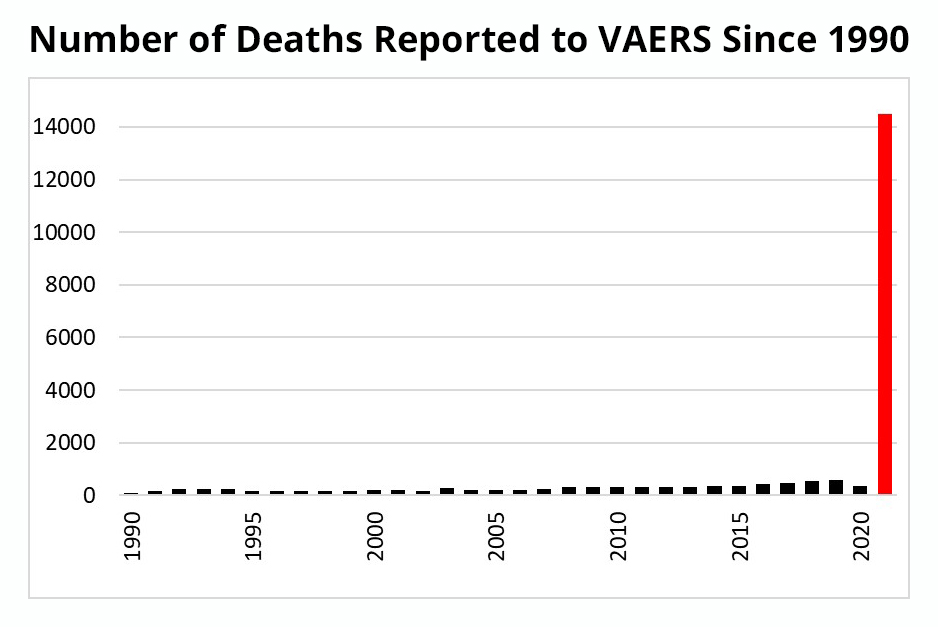
As of early September, there have been 14,506 deaths reported to VAERS for COVID-19 vaccines, compared to 8,673 for the preceding 30 years for all other vaccines. That is already more than 50 times the annual average — and we still have four months left to go until the end of the year.
It is hard to imagine how anyone can look at these numbers and not be at least a little bit concerned. Yet many people are dismissive, saying the unprecedented number of reports is due to the unprecedented number of vaccinations being administered.
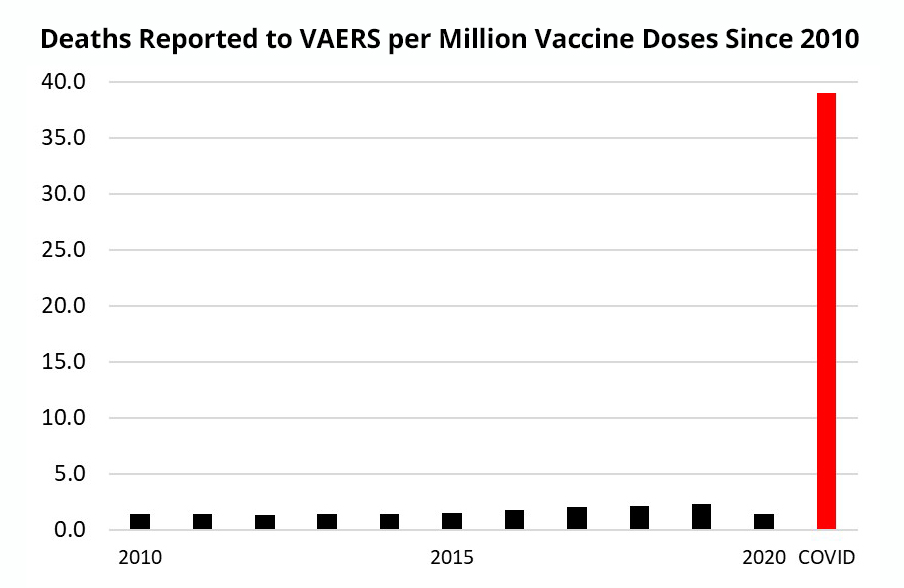
I crunched the numbers, and even after taking into account the total number of vaccinations, the number of reports for COVID vaccines still towers over previous years.
See, for example, Figure 2 below, which shows the number of deaths reported per million vaccine doses from 2010-2020 and for COVID-19 vaccines. That’s nearly 40 deaths reported per million COVID vaccines versus an average of 1.6 for all other vaccines from the previous 10 years.
No matter what I did to the data, or what types of adverse events I looked at, I could not make the big jump in COVID vaccine reports go away.
So why do the CDC and FDA not seem to be concerned about this? I don’t know, but to try to answer that question, we have to take a step back to talk about VAERS and how the CDC uses it to detect safety signals.
VAERS, which is jointly administered by the CDC and FDA, is typical of all reporting systems used to monitor the safety of medicinal products. Although widely used, there are many known limitations with this type of system. Probably the biggest is that it is passive or spontaneous, meaning it relies on the willingness of people and medical professionals to “spontaneously” submit reports. So reporting rates are low and inconsistent.
READ + SHARE my letter to Dr. Kessler, newly named co-chair of Biden’s #COVID-19 Advisory Committee, requesting he immediately fix Vaccine Adverse Event Reporting System (#VAERS), system that monitors adverse outcomes following vaccination. #TheDefenderhttps://t.co/Jw77i8NrOA
— Robert F. Kennedy Jr (@RobertKennedyJr) December 19, 2020
Another limitation is that reports cannot be used reliably to show a causal connection between a vaccine or medication and an adverse event. So what are they good for?
They are used to provide a kind of early warning system. When enough reports accumulate about a particular type of event, those reports produce a safety signal, like an alarm bell. When the alarm rings, it doesn’t mean there is definitely a problem, but it is supposed to alert authorities to a possible problem and prompt further investigation.
In late January, the CDC released a briefing document outlining the agency’s standard operating procedures for ongoing monitoring of VAERS for safety signals from COVID-19 vaccines.
The document lays out plans to produce weekly reports that would highlight any safety signals found across a range of different adverse events. Although those reports have not been made public, we don’t need to rely on the CDC, as VAERS data is publicly available.
To detect safety signals with new vaccines, I took my lead from a study published by CDC researchers who were trying to detect safety signals for the new H1N1 swine flu vaccines introduced in 2009. The researchers compared VAERS reports for H1N1 vaccines to reports for regular flu vaccines.
So I took a similar approach and compared adverse events reported for COVID-19 to events reported for flu vaccines. This comparison makes a lot of sense, as flu vaccines are the only other type of vaccine administered to adults and the elderly in large numbers.
Of course, because the number of flu and COVID-19 vaccines administered is not the same, it makes sense to look at the number of reports per dose administered, something not specified in the CDC briefing document.
Table 1 (below) shows a comparison of VAERS reports for COVID-19 vaccines versus flu vaccines per million doses administered for a range of different event types and age groups.
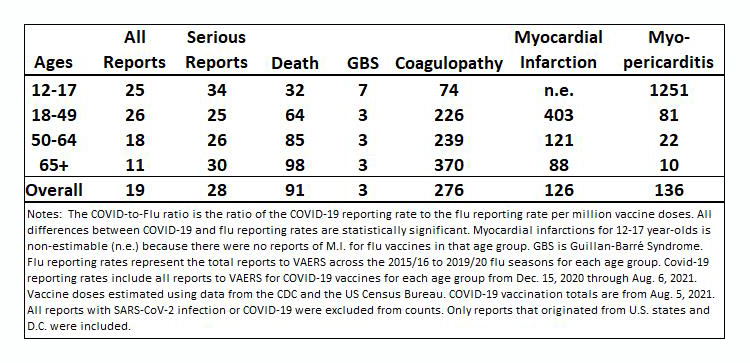
For each adverse event type, the table shows the COVID-to-Flu ratio, which simply shows how many more events were reported per million doses of COVID-19 vaccines compared to the number per million doses of seasonal influenza vaccines.
The comparison is based on all reports to VAERS following COVID-19 vaccines (from Dec. 15 – Aug. 6) to all reports for all seasonal influenza vaccines from the previous five influenza seasons (from 2015/16 to 2019/20).
Keep in mind that for all the analyses, I excluded all reports that came from people with an indication of a SARS-CoV-2 infection, such as a positive test result or even a suspicion of COVID-19 — so the adverse events can’t be blamed on that.
The first thing to notice is that for every type of adverse event for every age group, there were more reports per million doses of COVID-19 vaccines than for flu vaccines. If you look at the bottom row for all age groups (12 and older), you see that for every million vaccine doses administered, there were 19 times more reports to VAERS for COVID-19 vaccines than for flu vaccines, 28 times more serious events, 91 times more deaths, 3 times more reports of Guillain-Barré syndrome (GBS), 276 times more reports of coagulopathy; 126 times as many reports of myocardial infarction; and 136 times more reports of myopericarditis.
Also notable is the variation across age groups. For example, death and coagulopathy were more preponderant for older age groups, whereas GBS and myopericarditis were more frequent for younger age groups.
The ratios for myopericarditis put the full significance of these results into perspective, since it is an officially recognized side effect of COVID-19 vaccines, especially among men under age 50. (We used the reporting rates per million vaccine doses from that report, slide 30, to calculate the COVID-to-Flu ratios for myopericarditis, which were slightly smaller than our own calculations.) See for example this FDA press release and the below slide from an Aug. 30 CDC presentation to the ACIP:
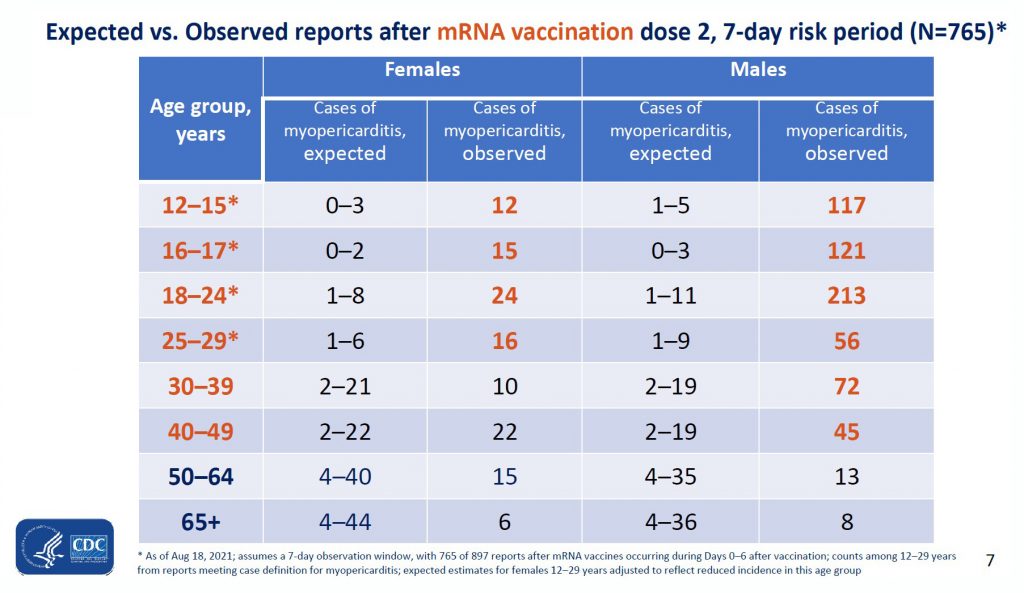
While the COVID-to-flu ratio for myopericarditis among 12- to 17-year-olds in Table 1 is in a league of its own at 1251-to-1, the ratio for the 18- to 49-year-olds is 81-to-1, which is well within the range of many of the other ratios in the table — and even smaller than many of them.
Because the CDC has acknowledged that mRNA COVID-19 vaccines can cause myocarditis in this age group, a reporting ratio of at least 81 is like an alarm bell going off to warn us of a potential safety problem. And the much larger ratios for coagulopathy and myocardial infarctions are like a 4-alarm fire.
So why does the CDC seem to be unconcerned about these safety signals? Is it possible they haven’t picked up on them?
Admittedly, comparing reports for COVID versus flu after taking the number of doses into account is not the same exact methodology anticipated in the CDC’s briefing document. Although it is arguably superior for a variety of reasons I won’t get into here, just to be sure I went ahead and did the exact same type of analysis outlined in the briefing document and found unambiguous safety signals.
Before showing the results, I need to explain how it works, but to do that we’ll have to get a bit deep in the weeds.
The method is a well-established pharmacovigilance technique based on calculating what’s known as the “Proportional Reporting Ratio” or PRR. To calculate the PRR, you first have to calculate the proportion of each type of event out of all events reported for that vaccine (COVID-19 and flu).
So for example, we take the number of VAERS reports of myocarditis for COVID-19 vaccines and divide that by the total number of all events reported for COVID-19 vaccines. Then we do the same for flu vaccines.
Then, to get the proportional reporting ratio (PRR), we divide the proportion of reports for a given type of event (like myopericarditis) for COVID-19 vaccines by the proportion for flu vaccines.
If the proportion for COVID-19 vaccines is large relative to the proportion for flu vaccines, that sends a signal alerting us to a potential safety problem. A safety signal is defined as a PRR that is greater than 2, statistically significant (with what’s known as a Chi-square value above 4) and has at least three of that type of event reported for each vaccine.
Table 2 below shows the PRR’s I calculated for several different adverse events across different age groups. All of the PRR’s in bold fit the CDC’s definition of a safety signal. This includes all PRR’s for death, except for the youngest age group, all PRR’s for coagulopathy and myopericarditis, and all PRR’s for myocardial infarction, except for the youngest age group because there were no myocardial infarctions reported for influenza vaccines.
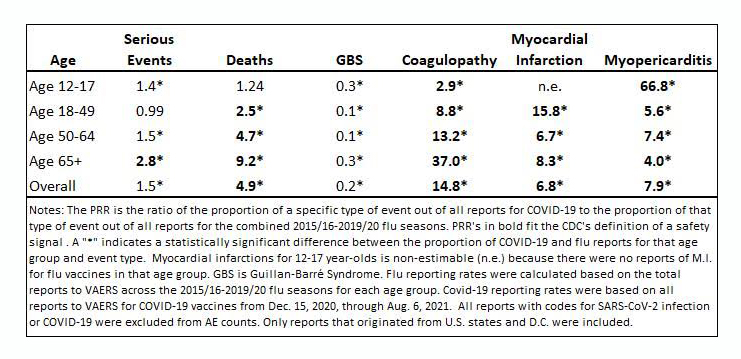
Note that, by default, the PRR method will never detect a safety signal for events that have never been reported for the comparator vaccine — like the zero teenage myocardial infarctions reported for flu vaccines ever compared to 10 for COVID-19 vaccines — which arguably should be seen as an even stronger indication that something is amiss.)
The only event that makes up a larger proportion of flu vaccine reports than COVID-19 vaccines is GBS.
Here, too, the PRRs for myopericarditis are instructive. Even though the PRR value for myopericarditis in the youngest age group is off the scale, the values for the 18 to 49 age group is similar to or even lower than the PRR’s for deaths, myocardial infarctions and coagulopathy.
Because the signal for myopericarditis is indicative of an actual, acknowledged safety problem, other signals of similar size might very well be alerting us to actual but unacknowledged problems.
I then went a step further and calculated PRRs for all adverse events submitted to VAERS. I found 242 adverse events that satisfied the definition of a safety signal according to the CDC.
Some of them were minor, like abnormal dreams or vaccination site discomfort. But many of them were very serious and included, in addition to the events shown in Table 2: cardiac arrests; cerebral hemorrhages; cerebrovascular accidents (strokes); renal failure; and vaginal hemorrhages — and that’s just the tip of the iceberg of serious events that show unambiguous safety signals.
An additional 87 types of events didn’t qualify as a safety signal just because they had been reported only once or twice for flu vaccines. An additional 6,159 types of events had never been reported for flu vaccines, despite more than 600 million flu vaccines administered among the age groups I examined.
For these events, it could be argued the safety signal is infinite, since the number of events in the denominator is zero. But instead of raising an alarm, they are by definition considered unworthy of concern.
No matter how I sliced and diced the data, the safety signal for COVID-19 vaccines rang loud and clear. It’s hard to imagine how anyone could miss it. It would be like taking a hike in Arizona and falling into the Grand Canyon because you didn’t see the big hole in the ground.
Some people are dismissive when presented with this evidence. “VAERS data can’t be trusted,” they say. “Anyone can submit a report and some of the reports are fraudulent.”
Yes, anybody can submit a report, and some might be fraudulent. But the CDC hasn’t raised any concerns about this and continues to use VAERS to monitor for safety signals.
A recent study found 67% of VAERS reports were submitted by healthcare workers, and the CDC confirmed that 88% of VAERS myopericarditis reports they examined fit their case definition.
Yes, VAERS is imperfect, but the large majority of reports are legitimate and reliable.
Another objection is that the increase in reporting is artificial. Many people are scared of these new vaccines. Awareness of VAERS is higher than it has ever been. And the government has actively encouraged, and in some cases required, people to report adverse events — so of course VAERS reports are going to increase.
But that doesn’t mean there are really more events. This phenomenon is known as “stimulated reporting.”
Nobody at any of the recent CDC advisory committee meetings raised any concern that VAERS reports were inflated. If the unprecedented increase in VAERS reports was just due to stimulated reporting, CDC researchers tell us we should expect to see COVID-to-flu ratios and PRRs that are roughly similar across different types of events. So if there was a 20-fold increase in reporting of serious events, say, then there should be a similar increase in other types of events.
A brief glance at Tables 1 and 2 clearly shows this is not the case — the reporting rates vary greatly across different types of events, and also across different age groups for the same event.
This is a huge giveaway that the increase — or at least a large portion of it — is not due to stimulated reporting. Indeed, underreporting is usually a bigger concern with data like VAERS, and there are good reasons to think the true number of adverse events is much larger.
But if the safety signal from VAERS is loud and clear and VAERS reports can be trusted, then how is the CDC not picking up on this? Or are they ignoring it? It’s hard to say.
It might have to do with how the CDC handles signals once they are detected. The agency’s protocols call for a thorough clinical review of events that trigger a safety signal in order to determine if the event could plausibly be caused by the vaccine. If that’s the case, it’s conceivable they found safety signals, but then determined that there was no plausible connection and therefore no cause for concern.
What this means in practice, however, is that if the CDC investigators do not understand how these novel vaccines — which use gene therapy technology and have had only limited use in humans — might cause a particular type of adverse event, the presumption is that there is no plausible connection.
For example, the CDC has declared after reviewing over 7,000 reports of deaths reported in the U.S. as of Sept. 7, they were not able to determine a plausible causal relationship for any of them, except for three due to thrombotic thrombocytopenic purpura (TTP) from the Janssen vaccine.
But the methods and criteria they use to make these determinations aren’t published anywhere, assuming they even exist. It would be easier to take their word for it if their decision-making process wasn’t hidden behind a veil of secrecy.
And maybe that’s the biggest problem of all: lack of transparency. VAERS reports are public, which is laudable, but what the CDC does with those reports is mostly hidden from view.
For example, the CDC briefing document outlining plans to monitor VAERS speaks of producing some dozen or more tables every week detailing the agency’s search for safety signals. To my knowledge, none of these have ever been made public.
And keep in mind that VAERS isn’t the only data source the CDC uses for safety monitoring. The other main source is the Vaccine Safety Datalink (VSD), which should be more reliable than VAERS because it uses patient medical records from some of the nation’s largest HMO’s.
There are several ongoing COVID-19 vaccine monitoring initiatives that use the VSD, including “COVID-19 Vaccine Safety Evaluation in Pregnant Women and their Infants,” “Mortality and Vaccination with COVID-19 Vaccines,” “COVID-19 Vaccine Safety, Spontaneous Abortion (SAB) and Stillbirth,” and “COVID-19 Vaccine-Mediated Enhanced Disease (VMED) and Vaccine Effectiveness.”
While these monitoring efforts are certainly praiseworthy, of the five that should have already started yielding initial results and interim reports, only partial results from two of them have been presented to the CDC advisory committee or made public in any way.
Where are the others? And how could forcing workers to get vaccinated ever be justified when so much of the evidence regarding their safety is still missing?
A complete and transparent accounting of the CDC’s safety monitoring is urgently needed, including internal communications and the results of all interim reports and analyses, whether through an Freedom of Information Act request, Congressional order or some other means.
The public deserves to know how the CDC reached the conclusion there was no plausible connection between the COVID-19 vaccines and the thousands of deaths they’ve reviewed, and also why they have failed to detect safety signals — or if they have, why they are being ignored.
Postscript: Since completing this article, I and others submitted comments to the meeting of FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) on Sept. 17, which voted 16 to 2 to not approve a booster dose for people under 65 years old, citing a lack of sufficient safety and efficacy data. However the FDA overruled its advisory committee, as did the CDC after its vaccine safety committee recommended against authorizing a third Pfizer dose for anyone other than people 65 and older, long-term care facility residents and certain people with underlying conditions.
© 2021 Children’s Health Defense, Inc. This work is reproduced and distributed with the permission of Children’s Health Defense, Inc. Want to learn more from Children’s Health Defense? Sign up for free news and updates from Robert F. Kennedy, Jr. and the Children’s Health Defense. Your donation will help to support us in our efforts.
Too Few Are Telling the Truth
Not long ago, conservative media was not beholden to anyone. Today, most sites are stuck on the Big Tech gravy train.
I’ll keep this short. The rise of Pandemic Panic Theater, massive voter fraud, and other “taboo” topics have neutered a majority of conservative news sites. You’ll notice they are very careful about what topics they tackle. Sure, they’ll attack Critical Race Theory, Antifa, and the Biden-Harris regime, but you won’t see them going after George Soros, Bill Gates, the World Economic Forum, or the Deep State, among others.
The reason is simple. They are beholden to Big Tech, and Big Tech doesn’t allow certain topics to be discussed or they’ll cut you off. Far too many conservative news outlets rely on Google, Facebook, and Twitter for the bulk of their traffic. They depend on big checks from Google ads to keep the sites running. I don’t necessarily hold it against them. We all do what we need to do to survive. I just wish more would do like we have, which is to cut out Big Tech altogether.
We don’t get Google checks. We don’t have Facebook or Twitter buttons on our stories. We don’t have a YouTube Channel (banned), and Instagram profile (never made one), or a TikTok (no thanks, CCO). We’re not perfect, but we’re doing everything we can to not owe anything to anyone… other than our readers. We owe YOU the truth. We owe YOU the facts that others won’t reveal about topics that others won’t tackle. And we owe America, this great land that allows us to take hold of these opportunities.
Like I said, I don’t hold other conservative sites under too much scrutiny over their choices. It’s easy for people to point fingers when we’re not the ones paying their bills or supporting their families. I just wish there were more who would break away. Today, only a handful of other major conservative news outlets have broken away from the Big Tech teat. Of course, we need help.
The best way you can help us grow and continue to bring proper news and opinions to the people is by donating. We appreciate everything, whether a dollar or $10,000. Anything brings us closer to a point of stability when we can hire writers, editors, and support staff to make the America First message louder. Our Giving Fuel page makes it easy to donate one-time or monthly. Alternatively, you can donate through PayPal or Bitcoin as well. Bitcoin: 3A1ELVhGgrwrypwTJhPwnaTVGmuqyQrMB8
Our network is currently comprised of nine sites:
- NOQ Report
- Conservative Playlist
- Truth. Based. Media.
- Freedom First Network
- Based Underground
- Uncanceled News
- American Conservative Movement
- Conservative Playbook
- Our Gold Guy
We are also building partnerships with great conservative sites like The Liberty Daily and The Epoch Times to advance the message as loudly as possible, and we’re always looking for others with which to partner.
Also, we could use contributions of content. If you write or want to start writing and you share our patriotic, conservative, America First ideology, contact us. The contact form on this and all pages on the site goes directly to me.
Some of our content is spread across multiple sites. Other pieces of content are unique. We write most of what we post but we also draw from those willing to allow us to share their quality articles, videos, and podcasts. We collect the best content from fellow conservative sites that give us permission to republish them. We’re not ego-driven; I’d much rather post a properly attributed story written by experts like Dr. Joseph Mercola or Natural News than rewrite it like so many outlets like to do. We’re not here to take credit. We’re here to spread the truth.
While donations are the best way to help, you can also support us by buying through our sponsors:
- MyPillow: Use promo code “NOQ” to get up to 66% off AND you’ll be helping a patriotic, America First company.
- Freedom Phone: Use promo code “MAGA” and get $50 off AND you’ll be helping a patriotic, America First company.
- OurGoldGuy: Tell them we sent you in your request to buy gold and it will help us… AND (wait for it) you’ll be helping a patriotic, America First company.
We know we could make a lot more money if we sold out like so many “conservative” publications out there. You won’t find Google ads on our site for a reason. Yes, they’re lucrative, but I don’t like getting paid by minions of Satan (I don’t like Google very much if you couldn’t tell).
Time is short. As the world spirals towards The Great Reset, the need for truthful journalism has never been greater. But in these times, we need as many conservative media voices as possible. Please help keep NOQ Report and the other sites in the network going. Our promise is this: We will never sell out America. If that means we’re going to struggle for a while or even indefinitely, so be it. Integrity first. Truth first. America first.
Thank you and God Bless,
JD Rucker
Bitcoin: 32SeW2Ajn86g4dATWtWreABhEkiqxsKUGn
With that said, our content may be reproduced and distributed as long as it has a link to the original source and the author is credited prominently. We don’t mind you using our content as long as you help out by giving us credit with a prominent link. If you feel like giving us a tip for the content, we will not object!
JD Rucker – EIC
@jdrucker